

Impact of smoking status on outcome in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention
- PMID: 22773074
- PMCID: PMC3459076
- DOI: 10.1007/s11239-012-0764-0
Impact of smoking status on outcome in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention
Abstract
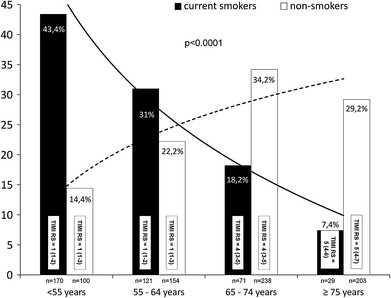
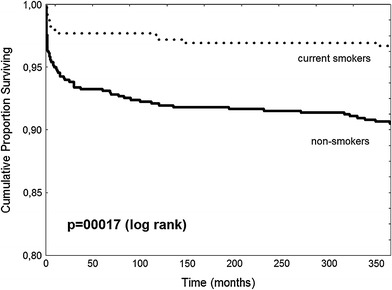
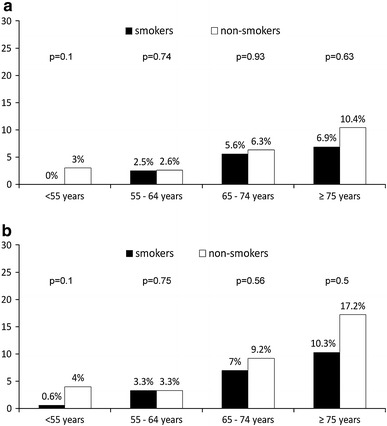
There are some data showing lower mortality of smokers comparing to non-smokers in patients with ST-segment elevation myocardial infarction (STEMI) when treated with thrombolysis or without reperfusion therapy. However, the role of smoking status is less established in patients with STEMI undergoing mechanical reperfusion. We evaluate the influence of smoking on outcome in patients with STEMI treated with primary percutaneous coronary intervention (PCI). A total of 1,086 patients enrolled into EUROTRANSFER Registry were included into present analysis. Patients were divided according to smoking status during STEMI presentation into those who were current smokers (391 patients, 36 %) and non-smokers (695 patients, 64 %). Current smokers were younger and more often men and less frequently had high-risk features as previous myocardial infarction, history of chronic renal failure, previous PCI, diabetes mellitus, anterior wall STEMI, and multivessel disease. Unadjusted mortality at 1 year was lower in current smokers comparing to non-smokers (3.3 vs. 9.5 %; OR 0.33 CI 0.18-0.6; p = 0.0001). However, after adjustment for age and gender by logistic regression, there was no longer significant difference between groups (OR 0.7; CI 0.37-1.36; p = 0.30). In conclusion, current smokers with STEMI treated with primary PCI have lower mortality at 1 year comparing to non-smokers, but this result may be explained by differences in baseline characteristics and not by smoking status itself. Current smokers developed STEMI more than 10 years earlier than non-smokers with similar age and sex-adjusted risk of death at 1 year. These results emphasize the role of efforts to encourage smoking cessation as prevention of myocardial infarction.
Figures
Similar articles
-
The impact of smoking on mortality after acute ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: a retrospective cohort outcome study at 3 years.J Thromb Thrombolysis. 2019 May;47(4):520-526. doi: 10.1007/s11239-019-01812-1. J Thromb Thrombolysis. 2019. PMID: 30666553
-
A retrospective cohort study of the association between smoking and mortality after acute ST-segment elevation myocardial infarction.Postgrad Med J. 2017 Aug;93(1102):489-493. doi: 10.1136/postgradmedj-2016-134605. Epub 2017 Mar 2. Postgrad Med J. 2017. PMID: 28254999
-
Clinical and angiographic profiles and six months outcomes of smokers with acute ST segment elevation myocardial infarction undergoing primary percutaneous coronary angioplasty.Indian Heart J. 2018 Sep-Oct;70(5):680-684. doi: 10.1016/j.ihj.2018.02.006. Epub 2018 Mar 12. Indian Heart J. 2018. PMID: 30392506 Free PMC article.
-
The enigma of the 'smoker's paradox': Results from a single-center registry of patients with STEMI undergoing primary percutaneous coronary intervention.Cardiovasc Revasc Med. 2024 Dec;69:42-49. doi: 10.1016/j.carrev.2024.06.007. Epub 2024 Jun 8. Cardiovasc Revasc Med. 2024. PMID: 38862370
-
Smoking is the dominating modifiable risk factor in younger patients with STEMI.Eur Heart J Acute Cardiovasc Care. 2020 Feb;9(1):70-75. doi: 10.1177/2048872618810414. Epub 2018 Nov 2. Eur Heart J Acute Cardiovasc Care. 2020. PMID: 30387680
Cited by
-
Differences in Angiographic Profile and Immediate Outcome of Primary Percutaneous Coronary Intervention in Otherwise Risk-Free Young Male Smokers.Cureus. 2020 Jun 24;12(6):e8799. doi: 10.7759/cureus.8799. Cureus. 2020. PMID: 32724746 Free PMC article.
-
Change in left ventricular systolic function in patients with ST elevation myocardial infarction: Evidence for smoker's paradox or pseudo-paradox?Indian Heart J. 2016 Nov-Dec;68(6):816-820. doi: 10.1016/j.ihj.2016.04.001. Epub 2016 Apr 14. Indian Heart J. 2016. PMID: 27931553 Free PMC article.
-
Smoking status and life expectancy after acute myocardial infarction in the elderly.Heart. 2016 Jan;102(2):133-9. doi: 10.1136/heartjnl-2015-308263. Epub 2015 Nov 23. Heart. 2016. PMID: 26596792 Free PMC article.
-
Smoking and 10-year risk of cardiovascular and non-cardiovascular events after contemporary coronary stenting.Am J Prev Cardiol. 2024 Aug 15;19:100718. doi: 10.1016/j.ajpc.2024.100718. eCollection 2024 Sep. Am J Prev Cardiol. 2024. PMID: 39247537 Free PMC article.
-
Effect of type D personality on smoking status and their combined impact on outcome after acute myocardial infarction.Clin Cardiol. 2018 Mar;41(3):321-325. doi: 10.1002/clc.22865. Epub 2018 Feb 19. Clin Cardiol. 2018. PMID: 29457844 Free PMC article.
References
-
- Kannel WB, Higgins M. Smoking and hypertension as predictors of cardiovascular risk in population studies. J Hypertens Suppl. 1990;8:S3–S8. - PubMed
-
- Barbash GI, White HD, Modan M, et al. Significance of smoking in patients receiving thrombolytic therapy for acute myocardial infarction. Experience gleaned from the International Tissue Plasminogen Activator/Streptokinase Mortality Trial. Circulation. 1993;87:53–58. doi: 10.1161/01.CIR.87.1.53. - DOI - PubMed
-
- Barbash GI, Reiner J, White HD, et al. Evaluation of paradoxic beneficial effects of smoking in patients receiving thrombolytic therapy for acute myocardial infarction: mechanism of the “smoker’s paradox” from the GUSTO-I trial, with angiographic insights. Global Utilization of Streptokinase and Tissue-Plasminogen Activator for Occluded Coronary Arteries. J Am Coll Cardiol. 1995;26:1222–1229. doi: 10.1016/0735-1097(95)00299-5. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
