

GLP-1 receptor activated insulin secretion from pancreatic β-cells: mechanism and glucose dependence
- PMID: 22776039
- PMCID: PMC3556522
- DOI: 10.1111/j.1463-1326.2012.01663.x
GLP-1 receptor activated insulin secretion from pancreatic β-cells: mechanism and glucose dependence
Abstract
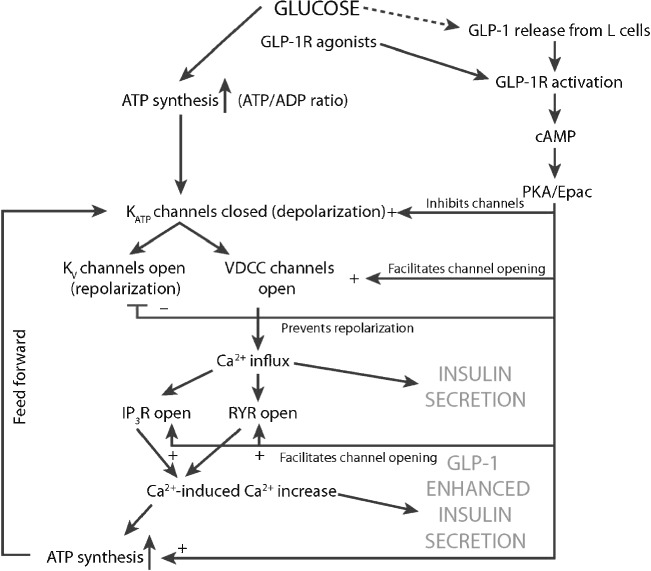
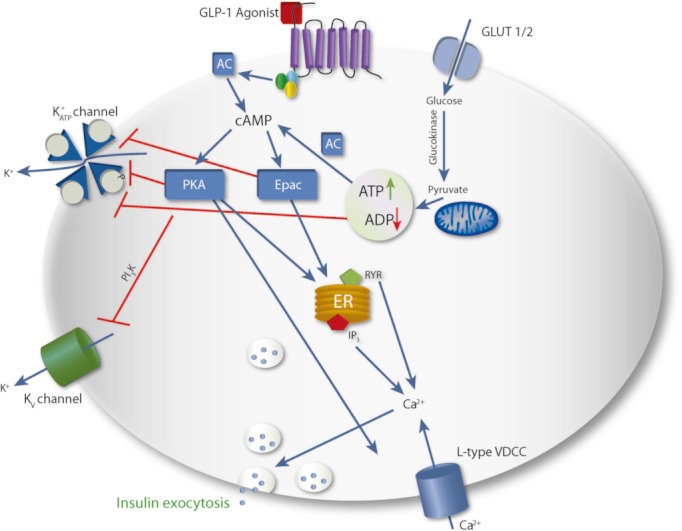
The major goal in the treatment of type 2 diabetes mellitus is to control the hyperglycaemia characteristic of the disease. However, treatment with common therapies such as insulin or insulinotrophic sulphonylureas (SU), while effective in reducing hyperglycaemia, may impose a greater risk of hypoglycaemia, as neither therapy is self-regulated by ambient blood glucose concentrations. Hypoglycaemia has been associated with adverse physical and psychological outcomes and may contribute to negative cardiovascular events; hence minimization of hypoglycaemia risk is clinically advantageous. Stimulation of insulin secretion from pancreatic β-cells by glucagon-like peptide 1 receptor (GLP-1R) agonists is known to be glucose-dependent. GLP-1R agonists potentiate glucose-stimulated insulin secretion and have little or no activity on insulin secretion in the absence of elevated blood glucose concentrations. This 'glucose-regulated' activity of GLP-1R agonists makes them useful and potentially safer therapeutics for overall glucose control compared to non-regulated therapies; hyperglycaemia can be reduced with minimal hypoglycaemia. While the inherent mechanism of action of GLP-1R agonists mediates their glucose dependence, studies in rats suggest that SUs may uncouple this dependence. This hypothesis is supported by clinical studies showing that the majority of events of hypoglycaemia in patients treated with GLP-1R agonists occur in patients treated with a concomitant SU. This review aims to discuss the current understanding of the mechanisms by which GLP-1R signalling promotes insulin secretion from pancreatic β-cells via a glucose-dependent process.
© 2012 Blackwell Publishing Ltd.
Figures
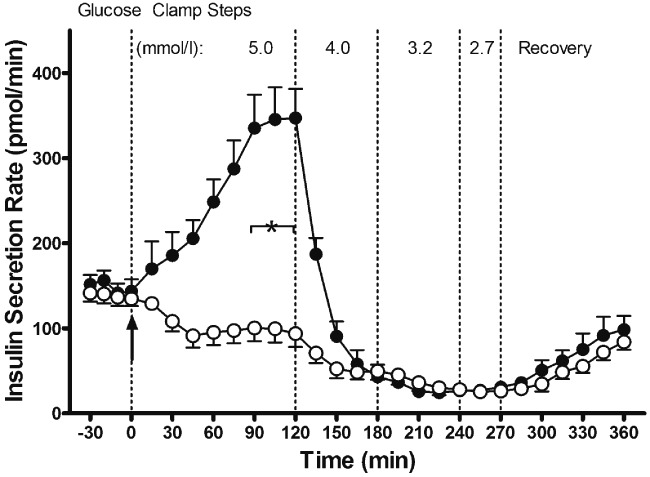
 , exenatide treatment arm. Data are means ± s.e.; n = 11 per treatment arm. *p < 0.05, exenatide vs. placebo during steady state of a glycaemic interval. Reproduced with permission from Degn et al. [31].
, exenatide treatment arm. Data are means ± s.e.; n = 11 per treatment arm. *p < 0.05, exenatide vs. placebo during steady state of a glycaemic interval. Reproduced with permission from Degn et al. [31].
References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetes Care. 2012;35:1577–1596. - PubMed
-
- Pettersson B, Rosenqvist U, Deleskog A, Journath G, Wändell P. Self-reported experience of hypoglycemia among adults with type 2 diabetes mellitus (Exhype) Diabetes Res Clin Pract. 2011;92:19–25. - PubMed
-
- Eckert B, Agardh CD. Hypoglycaemia leads to an increased QT interval in normal men. Clin Physiol. 1998;18:570–575. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
