

Associations between demographic, disease related, and treatment pathway related variables and health related quality of life in primary care patients with coronary heart disease
- PMID: 22776102
- PMCID: PMC3464887
- DOI: 10.1186/1477-7525-10-78
Associations between demographic, disease related, and treatment pathway related variables and health related quality of life in primary care patients with coronary heart disease
Abstract
Background: Coronary heart disease (CHD) is a common medical problem worldwide that demands shared care of general practitioners and cardiologists for concerned patients. In order to improve the cooperation between both medical specialists and to optimize evidence-based care, a treatment pathway for patients with CHD was developed and evaluated in a feasibility study according to the recommendation for the development and evaluation of complex interventions of the British Medical Research Council (MRC). In the context of this feasibility study the objective of the present research was to investigate the contributions of different disease related (e.g. prior myocardial infarction), pathway related (e.g. basic medication) and demographic variables on patients` perceived health related quality of life (HRQoL) as a relevant and widely used outcome measure in cardiac populations.
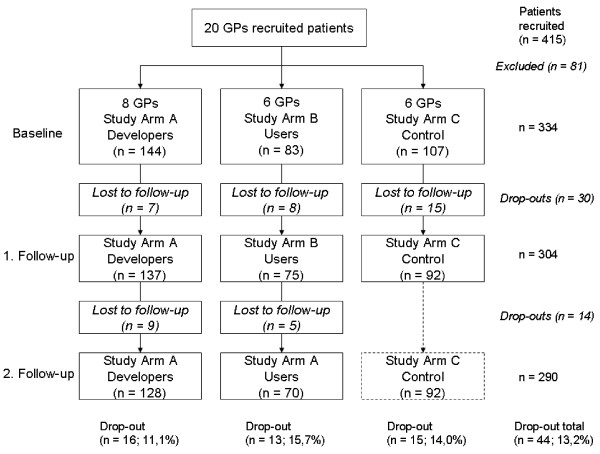
Methods: Data assessing demographic, disease and pathway related variables of CHD patients included in the study were collected in a quasi-experimental design with three study arms (pathway developers, users, control group) via case record forms and questionnaires at baseline and after 6 and 12 (intervention groups), and 9 months (control group), respectively after the initial implementation on GP level. Additionally, at the same measuring points the CHD patients participating in the study were interviewed by phone regarding their perceived HRQoL, measured with the EuroQol EQ-5D as an index-based health questionnaire. Due to the hierarchical structure of the data, we performed cross-sectional and longitudinal linear mixed models to investigate the impact of disease related, pathway related and demographic variables on patients` perceived HRQoL.
Results: Of 334 initially recruited patients with CHD, a total of 290 were included in our analysis. This was an average 13.2% dropout rate from baseline assessment to the 12-month follow-up. At all assessment points, patients` HRQoL was associated with a variety of sociodemographic variables (e.g. gender, employment, education) in each study group, but there was no association with pathway related variables. In both cross-sectional and longitudinal analyses highest HRQoL values in patients were reported in the physician group that had developed the pathway. In the longitudinal analyses there were no significant changes in the reported HRQoL values of the three groups over time.
Conclusions: The found associations between sociodemographic variables and the perceived HRQoL of patients with CHD are in line with other research. As there are no associations of HRQoL with pathway related variables like the basic medication, possible weaknesses in the study design or the choice of outcome have to be considered before planning and conducting an evaluation study according to the MRC recommendations. Additionally, as patients in the developer group reported the highest HRQoL values over time, a higher commitment of the GPs in the developer group can be assumed and should be considered in further research.
Figures


References
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. - PubMed
-
- Kesteloot H, Sans S, Kromhout D. Dynamics of cardiovascular and all-cause mortality in Western and Eastern Europe between 1970 and 2000. Eur Heart J. 2006;27(1):107–113. - PubMed
-
- Lange C, Ziese T. Daten und Fakten: Ergebnisse der Studie "Gesundheit in Deutschland aktuell 2009". Berlin: Robert Koch Institut; 2010.
-
- Hall JA, Horgan TG, Stein TS, Roter DL. Liking in the physician–patient relationship. Patient Educ Couns. 2002;48(1):69–77. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
