

Perioperative outcomes of severely obese children undergoing tonsillectomy
- PMID: 22776351
- PMCID: PMC3470734
- DOI: 10.1111/j.1460-9592.2012.03905.x
Perioperative outcomes of severely obese children undergoing tonsillectomy
Abstract
Background: Sleep-disordered breathing, a common condition in obese children, is a frequent indication for tonsillectomy.
Objective: The purpose of this study was to examine the association between obesity and perioperative complications in children undergoing tonsillectomy.
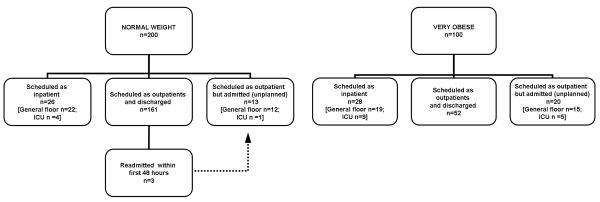
Methods/materials: A sample of 100 severely obese children (body mass index for age [BMIA], ≥ 98 th percentile) between ages 2 and 18 years who underwent tonsillectomy at Mayo Clinic Rochester was randomly selected. Each severely obese child was age (± 2 years) and sex matched to two normal weight children (BMIA between 25th and 75th percentiles) undergoing tonsillectomy during the study period, and their medical records were reviewed.
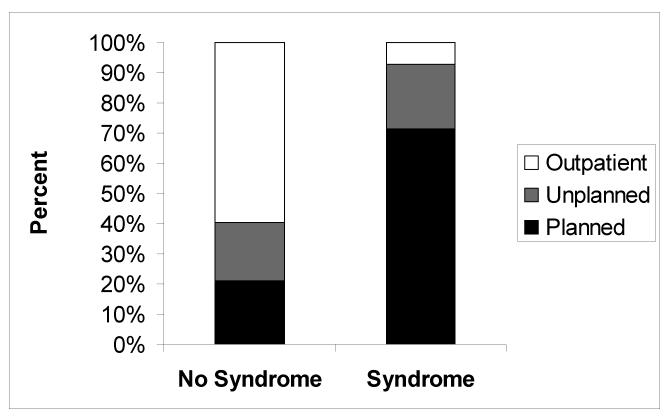
Results: Severely obese children had a significantly higher incidence of comorbid conditions including respiratory disorders and severe systemic disorders or syndromes. Severely obese children had a higher frequency of perioperative airway complications (15.0% vs 2.0%). From posthoc analyses, severe obesity remained a significant risk factor for perioperative adverse events after adjusting for the presence of severe systemic disorders or syndromes (OR 8.8; 95% CI 2.8-27.5, P < 0.001) and also after adjusting for preoperative respiratory disorders (OR 7.7; 95% CI 2.5-24.3, P < 0.001). When children with planned admissions were excluded from the analysis, severe obesity was associated with an increased rate of unplanned hospital admission (OR 3.80, 95% CI 1.8-7.9, P < 0.001).
Conclusions: Severe obesity in children undergoing tonsillectomy is independently associated with an increased risk of perioperative complications. It appears that both severe obesity and systemic comorbid condition contribute to higher proportions of inpatient tonsillectomies performed in our institution.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Baugh RF, Archer SM, Mitchell RB, et al. Clinical practice guideline: tonsillectomy in children. Otolaryngol Head Neck Surg. 2011;144:S1–30. - PubMed
-
- Blair RL, McKerrow WS, Carter NW, et al. The Scottish tonsillectomy audit. The Audit Sub-Committee of the Scottish Otolaryngological Society. J Laryngol Otol Suppl. 1996;20:1–25. - PubMed
-
- Erickson BK, Larson DR, St Sauver JL, et al. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970-2005. Otolaryngol Head Neck Surg. 2009;140:894–901. - PubMed
-
- Nafiu OO, Reynolds PI, Bamgbade OA, et al. Childhood body mass index and perioperative complications. Paediatr Anaesth. 2007;17:426–430. - PubMed
-
- Setzer N, Saade E. Childhood obesity and anesthetic morbidity. Paediatr Anaesth. 2007;17:321–326. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
