

Current management of massive hemorrhage in trauma
- PMID: 22776724
- PMCID: PMC3439269
- DOI: 10.1186/1757-7241-20-47
Current management of massive hemorrhage in trauma
Abstract
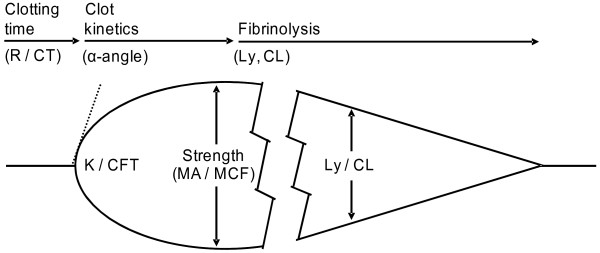
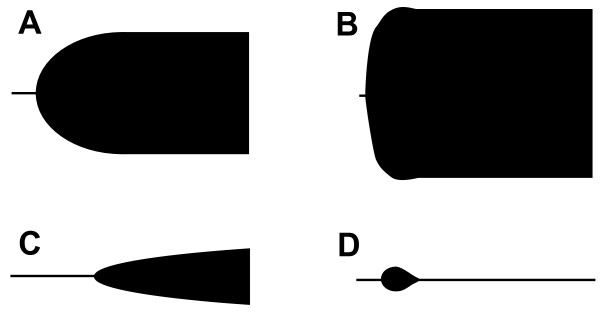
Hemorrhage remains a major cause of potentially preventable deaths. Trauma and massive transfusion are associated with coagulopathy secondary to tissue injury, hypoperfusion, dilution, and consumption of clotting factors and platelets. Concepts of damage control surgery have evolved prioritizing early control of the cause of bleeding by non-definitive means, while hemostatic control resuscitation seeks early control of coagulopathy.Hemostatic resuscitation provides transfusions with plasma and platelets in addition to red blood cells in an immediate and sustained manner as part of the transfusion protocol for massively bleeding patients. Although early and effective reversal of coagulopathy is documented, the most effective means of preventing coagulopathy of massive transfusion remains debated and randomized controlled studies are lacking. Viscoelastical whole blood assays, like TEG and ROTEM however appear advantageous for identifying coagulopathy in patients with severe hemorrhage as opposed the conventional coagulation assays.In our view, patients with uncontrolled bleeding, regardless of it's cause, should be treated with hemostatic control resuscitation involving early administration of plasma and platelets and earliest possible goal-directed, based on the results of TEG/ROTEM analysis. The aim of the goal-directed therapy should be to maintain a normal hemostatic competence until surgical hemostasis is achieved, as this appears to be associated with reduced mortality.
Figures
References
-
- Krausz MM. Fluid resuscitation strategies in the Israeli army. J Trauma. 2003;54:S39–S42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
