

Lay perspectives on hypertension and drug adherence: systematic review of qualitative research
- PMID: 22777025
- PMCID: PMC3392078
- DOI: 10.1136/bmj.e3953
Lay perspectives on hypertension and drug adherence: systematic review of qualitative research
Abstract
Objective: To synthesise the findings from individual qualitative studies on patients' understanding and experiences of hypertension and drug taking; to investigate whether views differ internationally by culture or ethnic group and whether the research could inform interventions to improve adherence.
Design: Systematic review and narrative synthesis of qualitative research using the 2006 UK Economic and Social Research Council research methods programme guidance.
Data sources: Medline, Embase, the British Nursing Index, Social Policy and Practice, and PsycInfo from inception to October 2011.
Study selection: Qualitative interviews or focus groups among people with uncomplicated hypertension (studies principally in people with diabetes, established cardiovascular disease, or pregnancy related hypertension were excluded).
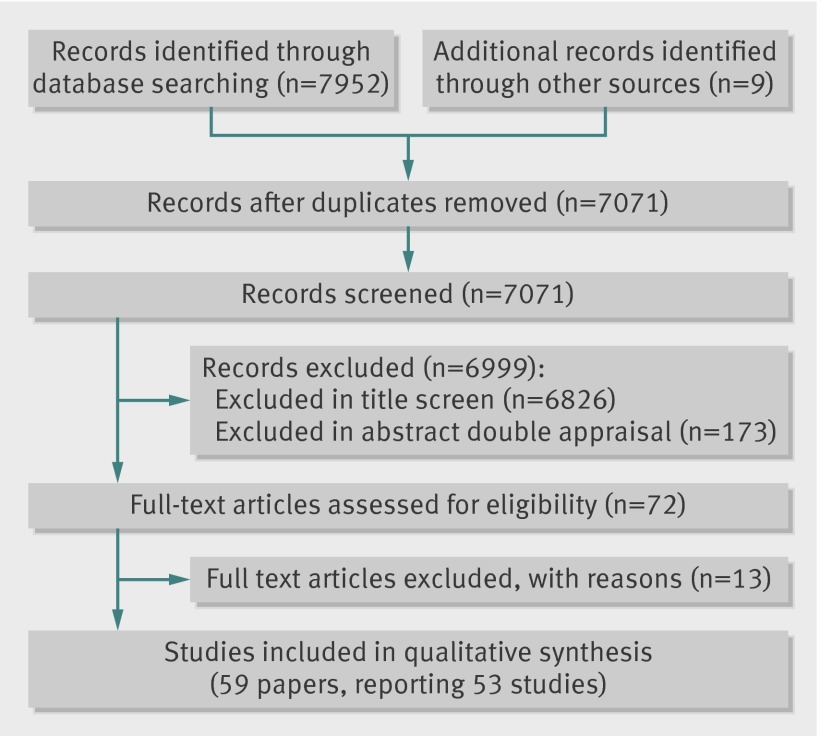
Results: 59 papers reporting on 53 qualitative studies were included in the synthesis. These studies came from 16 countries (United States, United Kingdom, Brazil, Sweden, Canada, New Zealand, Denmark, Finland, Ghana, Iran, Israel, Netherlands, South Korea, Spain, Tanzania, and Thailand). A large proportion of participants thought hypertension was principally caused by stress and produced symptoms, particularly headache, dizziness, and sweating. Participants widely intentionally reduced or stopped treatment without consulting their doctor. Participants commonly perceived that their blood pressure improved when symptoms abated or when they were not stressed, and that treatment was not needed at these times. Participants disliked treatment and its side effects and feared addiction. These findings were consistent across countries and ethnic groups. Participants also reported various external factors that prevented adherence, including being unable to find time to take the drugs or to see the doctor; having insufficient money to pay for treatment; the cost of appointments and healthy food; a lack of health insurance; and forgetfulness.
Conclusions: Non-adherence to hypertension treatment often resulted from patients' understanding of the causes and effects of hypertension; particularly relying on the presence of stress or symptoms to determine if blood pressure was raised. These beliefs were remarkably similar across ethnic and geographical groups; calls for culturally specific education for individual ethnic groups may therefore not be justified. To improve adherence, clinicians and educational interventions must better understand and engage with patients' ideas about causality, experiences of symptoms, and concerns about drug side effects.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Comment in
-
Hypertension: Understanding patients' perceptions could improve therapy.Nat Rev Cardiol. 2012 Sep;9(9):494. doi: 10.1038/nrcardio.2012.110. Epub 2012 Jul 24. Nat Rev Cardiol. 2012. PMID: 22825301 No abstract available.
References
-
- World Health Organization (WHO). The world health report 2002—reducing risks, promoting healthy life. 2011. www.who.int/whr/2002/en/. - PubMed
-
- Falaschetti E, Chaudhury M, Mindell J, Poulter N. Continued improvement in hypertension management in England: results from the Health Survey for England 2006. Hypertension 2009;53480-6. - PubMed
-
- Antikainen RL, Kastarinen MJ, Jousilahti P, Peltonen M, Laatikainen T, Beckett N, et al. Despite evidence-based guidelines, systolic blood pressure remains inadequately controlled in older hypertensive adults. J Hum Hypertens 2010;24:439-46. - PubMed
-
- Hart PD, Bakris GL. Hypertension control rates: time for translation of guidelines into clinical practice. Am J Med 2004;117:62-4. - PubMed
-
- World Health Organization. Adherence to long-term therapies: evidence for action. 2010. www.who.int/chp/knowledge/publications/adherence_report/en/index.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical