

Evaluation of clinical outcomes in patients with bloodstream infections due to Gram-negative bacteria according to carbapenem MIC stratification
- PMID: 22777044
- PMCID: PMC3421845
- DOI: 10.1128/AAC.06365-11
Evaluation of clinical outcomes in patients with bloodstream infections due to Gram-negative bacteria according to carbapenem MIC stratification
Abstract
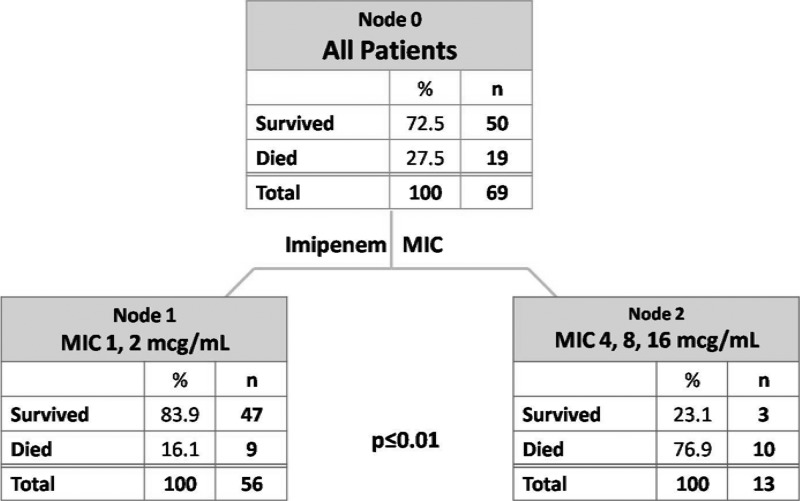
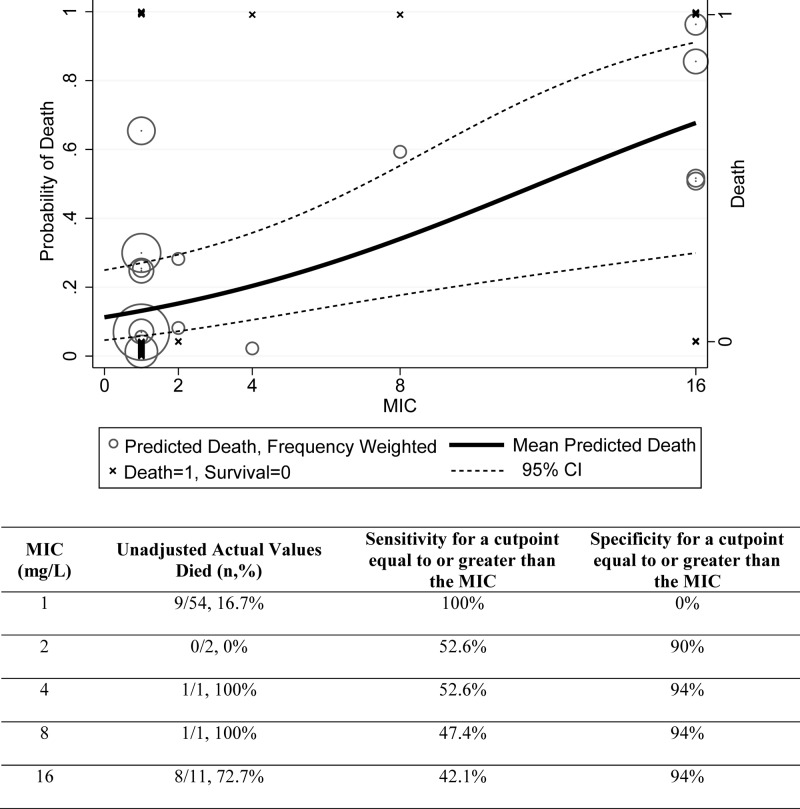
Predictive modeling suggests that actual carbapenem MIC results are more predictive of clinical patient outcomes than categorical classification of the MIC as susceptible, intermediate, or resistant. Some have speculated that current CLSI guidelines' suggested thresholds are too high and that clinical success is more likely if the MIC value is ≤1 mg/liter for certain organisms. Patients treated with carbapenems and with positive blood cultures for Pseudomonas aeruginosa, Acinetobacter baumannii, or extended-spectrum beta-lactamase (ESBL)-producing Gram-negative bacteria were considered for evaluation in this clinical retrospective cohort study. Relevant patient demographics and microbiologic variables were collected, including carbapenem MIC. The primary objective was to define a risk-adjusted all-cause hospital mortality breakpoint for carbapenem MICs. Secondarily, we sought to determine if a similar breakpoint existed for indirect outcomes (e.g., time to mortality and length of stay [LOS] postinfection for survivors). Seventy-one patients met the criteria for study inclusion. Overall, 52 patients survived, and 19 died. Classification and regression tree (CART) analysis determined a split of organism MIC between 2 and 4 mg/liter and predicted differences in mortality (16.1% versus 76.9%; P < 0.01). Logistic regression controlling for confounders identified each imipenem MIC doubling dilution as increasing the probability of death 2-fold (adjusted odds ratio [aOR] 2.0; 95% confidence interval [CI], 1.3 to 3.2). Secondary outcomes were similar between groups. This study revealed that patients with organisms that had a MIC of ≥4 mg/liter had worse outcomes than patients whose isolates had a MIC of ≤2 mg/liter, even after adjustment for confounding variables. We recommend additional clinical studies to better understand the susceptibility breakpoint for carbapenems.
Figures
References
-
- Ambrose PG, Bhavnani SM, Jones RN, Craig WA, Dudley MN. 2004. Use of pharmacokinetic-pharmacodynamic and Monte Carlo simulation as decision support for the re-evaluation of NCCLS cephem susceptibility breakpoints for Enterobacteriaceae, abstr A-138. Abstr. 44th Intersci. Conf. Antimicrob. Agents Chemother
-
- Bhavnani SM, Ambrose PG, Craig WA, Dudley MN, Jones RN. 2006. Outcomes evaluation of patients with ESBL- and non-ESBL-producing Escherichia coli and Klebsiella species as defined by CLSI reference methods: report from the SENTRY Antimicrobial Surveillance Program. Diagn. Microbiol. Infect. Dis. 54:231–236 - PubMed
-
- Bhavnani SM, et al. 2010. Pharmacokinetic-pharmacodynamic basis for CLSI carbapenem susceptibility breakpoint changes, abstr A-1382. Abstr. 50th Intersci. Conf. Antimicrob. Agents Chemother
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
