

Feasibility of a fixed-dose regimen of pyrazinamide and its impact on systemic drug exposure and liver safety in patients with tuberculosis
- PMID: 22777045
- PMCID: PMC3486525
- DOI: 10.1128/AAC.05988-11
Feasibility of a fixed-dose regimen of pyrazinamide and its impact on systemic drug exposure and liver safety in patients with tuberculosis
Abstract
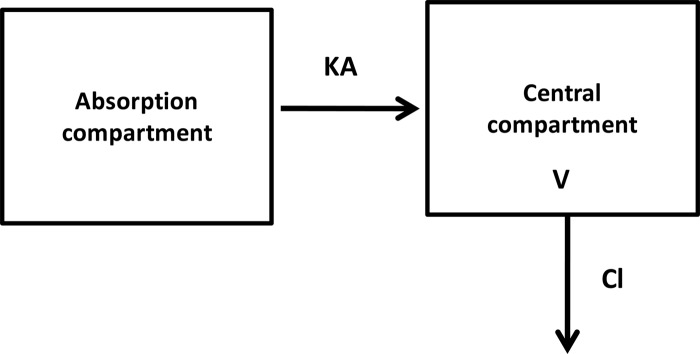
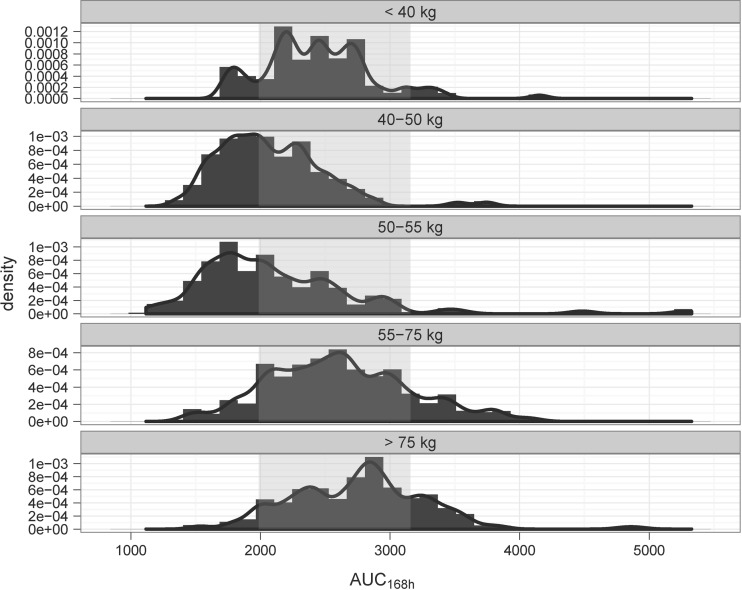
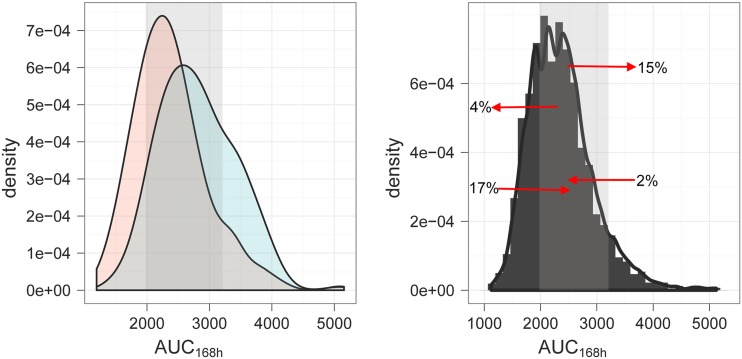
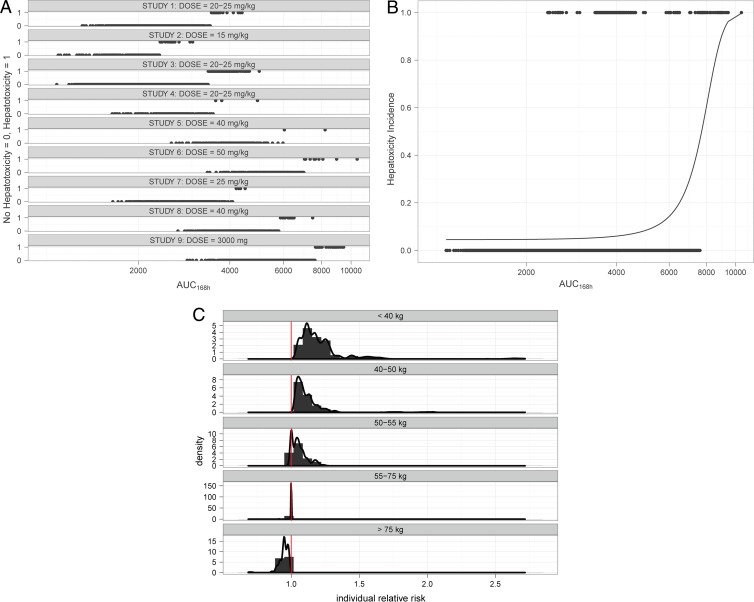
Historically, dosing regimens for the treatment of tuberculosis (TB) have been proposed in an empirical manner. Dose selection has often been the result of efficacy trials in which drugs were administered regardless of the magnitude of the effect of demographic factors on drug disposition. This has created challenges for the prescription of fixed-dose combinations with novel therapeutic agents. The objectives of this investigation were to evaluate the impact of body weight on the overall systemic exposure to pyrazinamide (PZA) and to assess whether the use of one fixed dose, without adjustment according to weight, would ensure target exposure and safety requirements across the overall patient population. Using a population pharmacokinetic model, simulation scenarios were explored based on population demographics from clinical trials in TB patients and on historical hepatotoxicity data. The systemic drug exposure (area under the concentration-time curve [AUC]), peak concentrations (the maximum concentration of drug in serum [C(max)]), the time above the MIC (t > MIC), and the risk of hepatotoxicity were evaluated for the current weight-banded regimen and compared to fixed doses under the assumption that pharmacokinetic differences are the primary drivers of toxicity. Evaluation of the standard weight banding reveals that more than 50% of subjects in the weight range of 45 to 55 kg remain below the proposed target exposure to PZA. In contrast, the use of a fixed 1,500-mg dose resulted in a lower proportion of subjects under the target value, with a 0.2% average overall increase in the risk of hepatotoxicity. Our results strongly support the use of a fixed-dose regimen for PZA in coformulation or combination with novel therapeutic agents.
Figures
References
-
- Acocella G, Angel JH. 1986. Short-course chemotherapy of pulmonary tuberculosis: a new approach to drug dosage in the initial intensive phase. Am. Rev. Respir. Dis. 134:1283–1286 - PubMed
-
- Acocella G, et al. 1993. Bioavailability of isoniazid, rifampicin and pyrazinamide (in free combination or fixed-triple formulation) in intermittent antituberculous chemotherapy. Monaldi Arch. Chest Dis. 48:205–209 - PubMed
-
- Agrawal S, et al. 2004. Comparative bioavailability of rifampicin, isoniazid and pyrazinamide from a four drug fixed dose combination with separate formulations at the same dose levels. Int. J. Pharm. 276:41–49 - PubMed
-
- Angel JH, Somner AR, Citron MK. 1979. Toxicity of antituberculosis drugs with special reference to hepatotoxicity. Bull. Int. Union Tuberc. 54:47–48
-
- Baghaei P, et al. 2010. Incidence, clinical and epidemiological risk factors, and outcome of drug-induced hepatitis due to antituberculous agents in new tuberculosis cases. Am. J. Ther. 17:17–22 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
