

Analysis of risk factors for lymph nodal involvement in early stages of rectal cancer: when can local excision be considered an appropriate treatment? Systematic review and meta-analysis of the literature
- PMID: 22778940
- PMCID: PMC3388331
- DOI: 10.1155/2012/438450
Analysis of risk factors for lymph nodal involvement in early stages of rectal cancer: when can local excision be considered an appropriate treatment? Systematic review and meta-analysis of the literature
Abstract
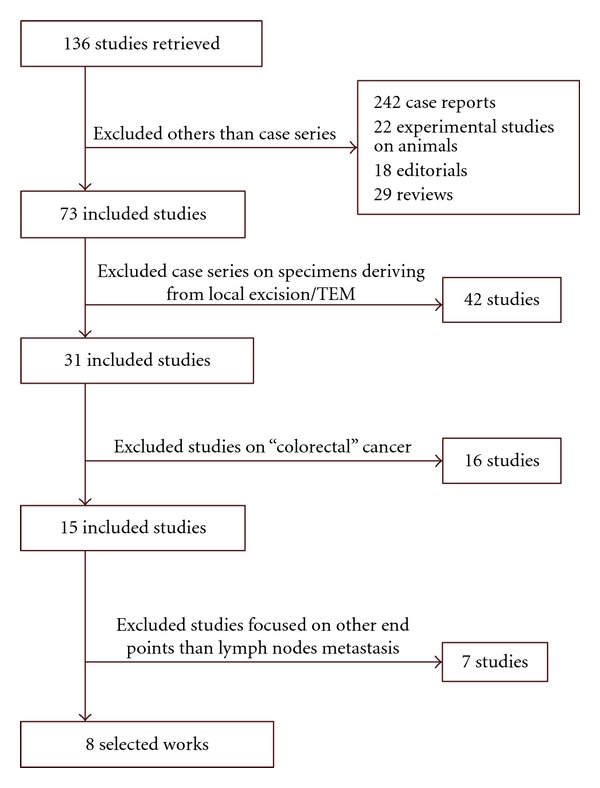
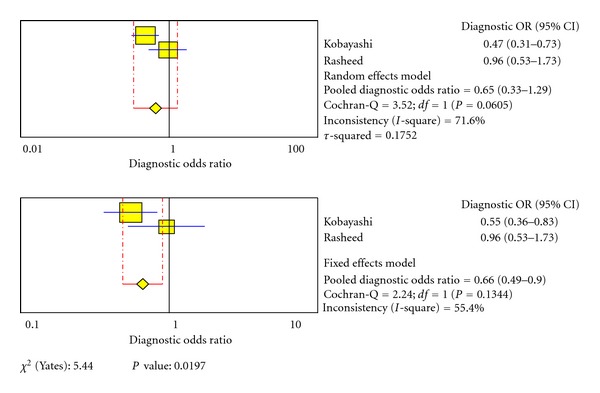
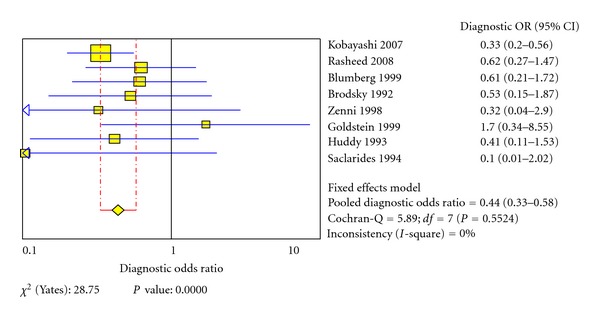
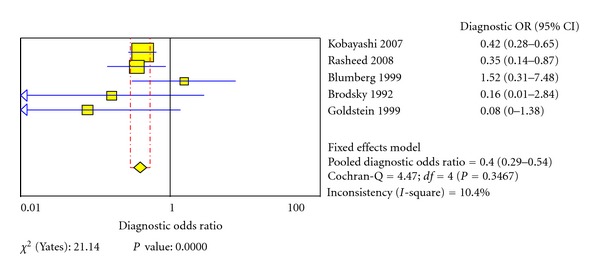
Background. Over the past ten years oncological outcomes achieved by local excision techniques (LETs) as the sole treatment for early stages of rectal cancer (ESRC) have been often disappointing. The reasons for these poor results lie mostly in the high risk of the disease's diffusion to local-regional lymph nodes even in ESRC. Aims. This study aims to find the correct indications for LET in ESRC taking into consideration clinical-pathological features of tumours that may reduce the risk of lymph node metastasis to zero. Methods. Systematic literature review and meta-analysis of casistics of ESRC treated with total mesorectal excision with the aim of identifying risk factors for nodal involvement. Results. The risk of lymph node metastasis is higher in G ≥ 2 and T ≥ 2 tumours with lymphatic and/or vascular invasion. Other features which have not yet been sufficiently investigated include female gender, TSM stage >1, presence of tumour budding and/or perineural invasion. Conclusions. Results comparable to radical surgery can be achieved by LET only in patients with T(1) N(0) G(1) tumours with low-risk histological features, whereas deeper or more aggressive tumours should be addressed by radical surgery (RS).
Figures
Similar articles
-
Risk factors for nodal involvement in early-stage rectal cancer: a new scoring system based on the analysis of 326 cases.Minerva Surg. 2022 Oct;77(5):448-454. doi: 10.23736/S2724-5691.21.08940-1. Epub 2021 Aug 2. Minerva Surg. 2022. PMID: 34338462
-
Small carcinomas involving less than one-quarter of the rectal circumference: local excision is still associated with a high risk of nodal positivity.Colorectal Dis. 2015 Oct;17(10):876-81. doi: 10.1111/codi.12953. Colorectal Dis. 2015. PMID: 25808035
-
Can depth of tumour invasion predict lymph node positivity in patients undergoing resection for early rectal cancer? A comparative study between T1 and T2 cancers.Colorectal Dis. 2008 Mar;10(3):231-8. doi: 10.1111/j.1463-1318.2007.01411.x. Colorectal Dis. 2008. PMID: 18257848
-
Outcome of lateral pelvic lymph node dissection with total mesorectal excision in treatment of rectal cancer: A systematic review and meta-analysis.Surgery. 2021 May;169(5):1005-1015. doi: 10.1016/j.surg.2020.11.010. Epub 2020 Dec 13. Surgery. 2021. PMID: 33317903
-
Diagnosis and treatment of invasive squamous cell carcinoma of the skin: European consensus-based interdisciplinary guideline.Eur J Cancer. 2015 Sep;51(14):1989-2007. doi: 10.1016/j.ejca.2015.06.110. Epub 2015 Jul 25. Eur J Cancer. 2015. PMID: 26219687 Review.
Cited by
-
TransAnal Minimally Invasive Surgery (TAMIS) with SILS™ port versus Transanal Endoscopic Microsurgery (TEM): a comparative experimental study.Surg Endosc. 2013 Oct;27(10):3762-8. doi: 10.1007/s00464-013-2962-z. Epub 2013 May 1. Surg Endosc. 2013. PMID: 23636523 Review.
-
Endoscopic Submucosal Dissection (ESD) in Colorectal Tumors.Viszeralmedizin. 2014 Feb;30(1):39-44. doi: 10.1159/000358529. Viszeralmedizin. 2014. PMID: 26288580 Free PMC article. Review.
-
Excision of malignant and pre-malignant rectal lesions by transanal endoscopic microsurgery in patients under 50 years of age.World J Gastrointest Surg. 2023 Sep 27;15(9):1892-1900. doi: 10.4240/wjgs.v15.i9.1892. World J Gastrointest Surg. 2023. PMID: 37901725 Free PMC article.
-
Multidisciplinary Treatment Strategy for Early Colon Cancer: A Review-An English Version.J Anus Rectum Colon. 2022 Oct 27;6(4):203-212. doi: 10.23922/jarc.2022-046. eCollection 2022. J Anus Rectum Colon. 2022. PMID: 36348951 Free PMC article. Review.
-
A novel opportunity in minimally invasive colorectal cancer therapy: defining a role for endoscopic submucosal dissection in the United States.Diagn Ther Endosc. 2013;2013:681783. doi: 10.1155/2013/681783. Epub 2013 Nov 6. Diagn Ther Endosc. 2013. PMID: 24319325 Free PMC article. Review.
References
-
- Frattini M, Balestra D, Suardi S, et al. Different genetic features associated with colon and rectal carcinogenesis. Clinical Cancer Research. 2004;10(12):4015–4021. - PubMed
-
- Ikeda Y, Mori M, Akagi K, et al. Differences between features of adenoma in the rectum versus sigmoid colon. American Journal of Gastroenterology. 2000;95(12):3620–3623. - PubMed
-
- Kapiteijn E, Liefers GJ, Los LC, et al. Mechanisms of oncogenesis in colon versus rectal cancer. Journal of Pathology. 2001;195(2):171–178. - PubMed
-
- Kobayashi H, Mochizuki H, Sugihara K, et al. Characteristics of recurrence and surveillance tools after curative resection for colorectal cancer: a multicenter study. Surgery. 2007;141(1):67–75. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
