

doi: 10.5402/2012/412896.
Epub 2012 Jun 21.
Orbital IgG4-Related Disease: Clinical Features and Diagnosis
Affiliations
- PMID: 22778989
- PMCID: PMC3388428
- DOI: 10.5402/2012/412896
Item in Clipboard
Orbital IgG4-Related Disease: Clinical Features and Diagnosis
ISRN Rheumatol.
2012.
Abstract
Orbital IgG4-related disease, which can occur in adults of any age, is characterized by IgG4-positive lymphoplasmacytic infiltrations in ocular adnexal tissues. The signs and symptoms include chronic noninflammatory lid swelling and proptosis. Patients often have a history of allergic disease and elevated serum levels of IgG4 and IgE as well as hypergammaglobulinemia. Orbital IgG4-related disease must be differentiated from idiopathic orbital inflammation and ocular adnexal marginal zone B-cell lymphoma to ensure appropriate and effective treatment. Systemic steroid therapy decreases the size of the lesions, but relapse often occurs when systemic steroid therapy is discontinued.
Figures
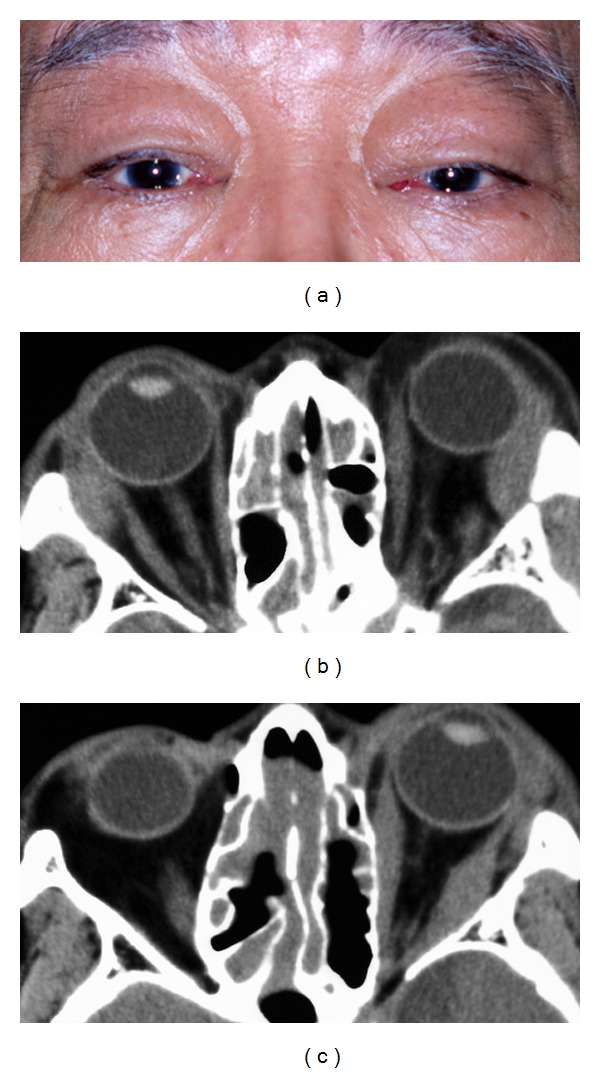
A typical case of orbital IgG4-related disease. A 72-year-old man with bilateral upper eyelid swellings that developed over a one-year period (a). There was a 10-year history of chronic rhinosinusitis, and the patients had undergone surgical treatments. On examination, his best-corrected visual acuity was 20/20 OD and 20/25 OS. Computed tomography showed enlargements of both lacrimal glands (b), enlargement of several of the left extraocular muscles (c), and infiltrative lesions in the ethmoid and maxillary sinuses. However, his ocular movements were unrestricted, and diplopia was not observed. He had elevated levels of serum IgG (4205 mg/dL; normal range: 870–1700 mg/dL) and serum IgG4 (1190 mg/dL; normal range: 4.8–105 mg/dL). These infiltrative lesions decreased in size after administration of oral prednisolone (30 mg) with a slow taper.
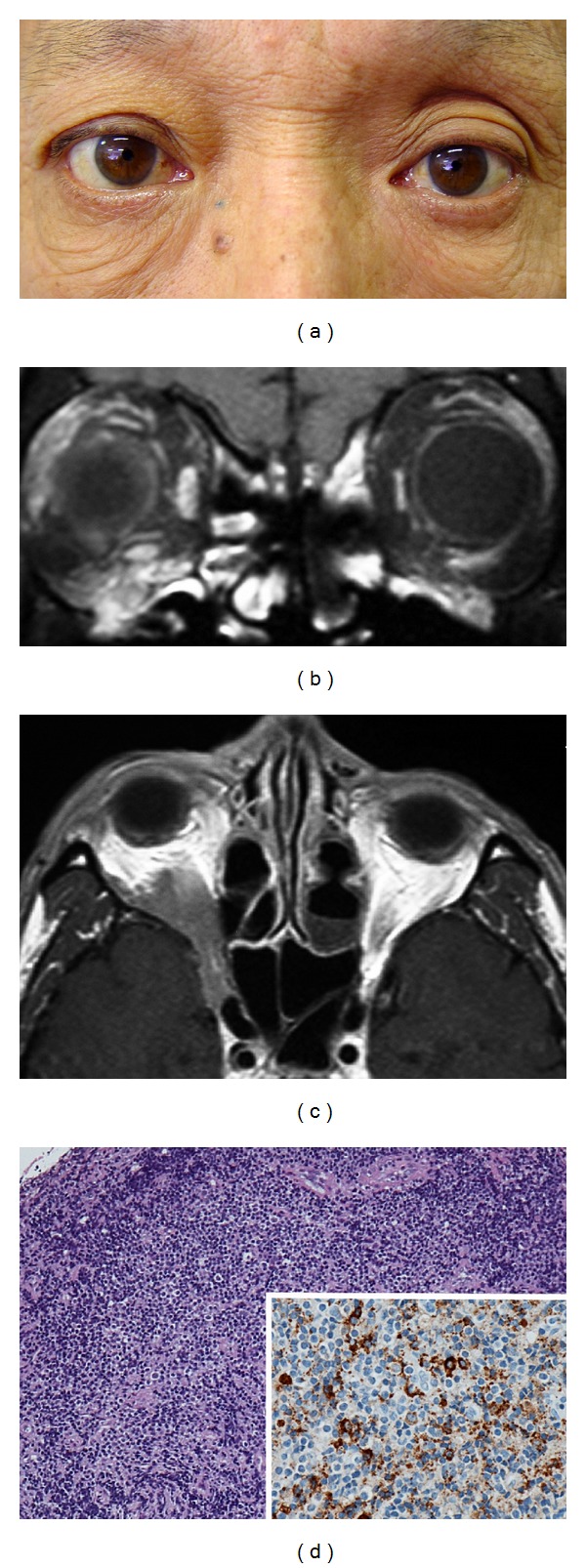
An extraorbital extension of orbital IgG4-related disease. This 60-year-old man presented with visual field defects in the right eye during a one-month period. On examination, his best-corrected visual acuity was 20/20 OD and 20/12.5 OS. Humphrey 30-2 threshold perimetry on his right eye showed an inferior altitudinal defect. He had 4 mm proptosis in the right eye (a). Magnetic resonance imaging of the brain and orbits with gadolinium showed infiltrative lesions in the right inferior orbit, infraorbital nerves (b), and also in the orbital apex and cavernous sinus (c). Clinical findings and imaging studies suggested compressive optic neuropathy. He had an elevated level of serum IgG4 (223 mg/dL; normal range: 4.8–105 mg/dL). Biopsy specimens showed lymphoproliferative lesions with IgG4-positive plasma cells and focal sclerosis (d). These findings were consistent with orbital IgG4-related disease with an extraorbital extension.
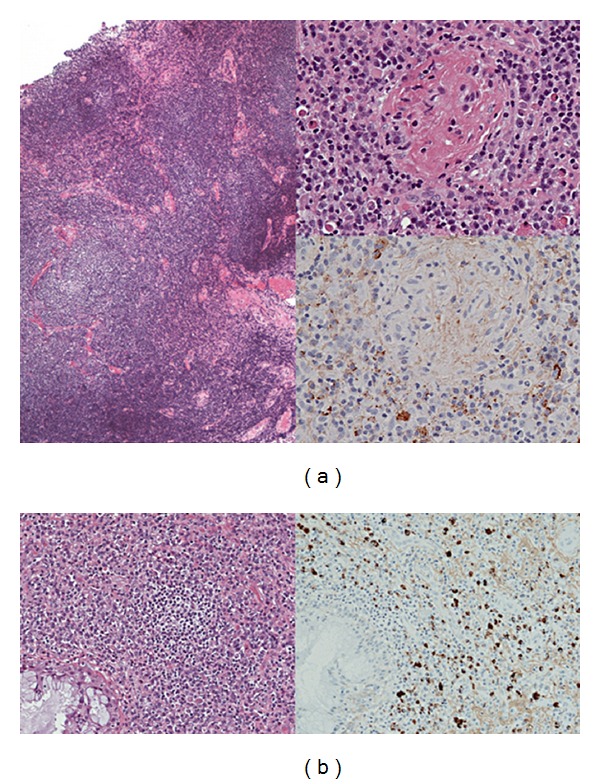
Histological findings in a typical case of orbital IgG4-related disease. Biopsy specimens from the patient in Figure 1 showed reactive lymphoid hyperplasia with plasma cells in the left lacrimal gland (a) and intensive lymphoplasmacytic infiltrations with IgG4-positive plasma cells in the ethmoid sinus (b). Immunostaining for IgG4 showed IgG4-positive plasma cells in the left lacrimal gland (top insert) and also in the ethmoid sinus (bottom, right).
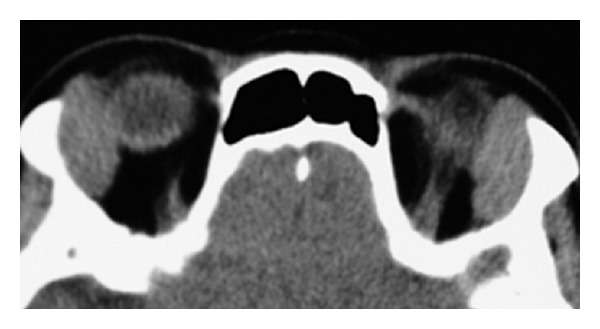
An unrelated case with symptoms similar to orbital IgG4-related disease. This 71-year-old woman had a 6-month history of swelling of both upper eyelids. Computed tomography showed an enlargement of both lacrimal glands. Histology and immunohistochemistry showed reactive lymphoid hyperplasia without IgG4-positive plasma cells. The woman had normal level of IgG4 (57 mg/dL) and an indolent clinical course for two years without treatments.
References
-
- Yamamoto M, Takahashi H, Sugai S, Imai K. Clinical and pathological characteristics of Mikulicz’s disease. Autoimmunity Reviews. 2005;4(4):195–200. - PubMed
-
- Takahira M, Kawano M, Zen Y, Minato H, Yamada K, Sugiyama K. IgG4-related chronic sclerosing dacryoadenitis. Archives of Ophthalmology. 2007;125(11):1575–1578. - PubMed
-
- Kubota T, Moritani S, Katayama M, Terasaki H. Ocular adnexal IgG4-related lymphoplasmacytic infiltrative disorder. Archives of Ophthalmology. 2010;128(5):577–584. - PubMed
-
- Plaza JA, Garrity JA, Dogan A, Ananthamurthy A, Witzig TE, Salomão DR. Orbital inflammation with IgG4-positive plasma cells: manifestation of IgG4 systemic disease. Archives of Ophthalmology. 2011;129(4):421–428. - PubMed
-
- Sato Y, Ohshima KI, Ichimura K, et al. Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathology International. 2008;58(8):465–470. - PubMed
LinkOut - more resources
Full Text Sources
