

Linking the Tinnitus Questionnaire and the subjective Clinical Global Impression: which differences are clinically important?
- PMID: 22781703
- PMCID: PMC3487915
- DOI: 10.1186/1477-7525-10-79
Linking the Tinnitus Questionnaire and the subjective Clinical Global Impression: which differences are clinically important?
Abstract
Background: Development of new tinnitus treatments requires prospective placebo-controlled randomized trials to prove their efficacy. The Tinnitus Questionnaire (TQ) is a validated and commonly used instrument for assessment of tinnitus severity and has been used in many clinical studies. Defining the Minimal Clinically Important Difference (MCID) for TQ changes is an important step to a better interpretation of the clinical relevance of changes observed in clinical trials. In this study we aimed to estimate the minimum change of the TQ score that could be considered clinically relevant.
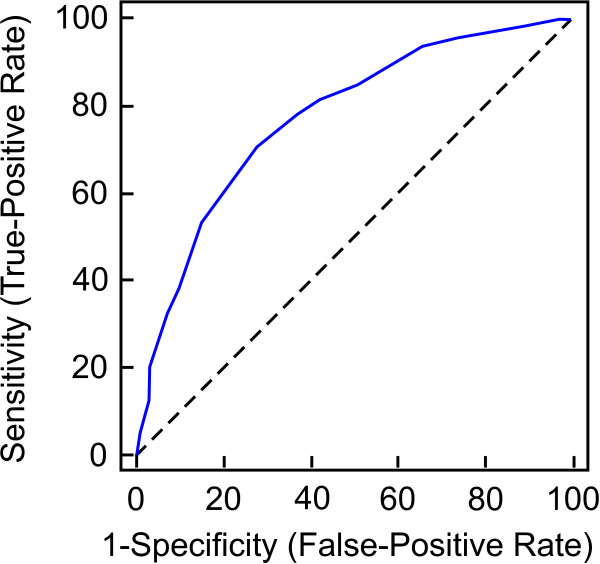
Methods: 757 patients with chronic tinnitus were pooled from the TRI database and the RESET study. An anchor-based approach using the Clinical Global Impression (CGI) scale and distributional approaches were used to estimate MCID. Receiver Operating Characteristic (ROC) curves were calculated to define optimal TQ change cutoffs discriminating between minimally changed and unchanged subjects.
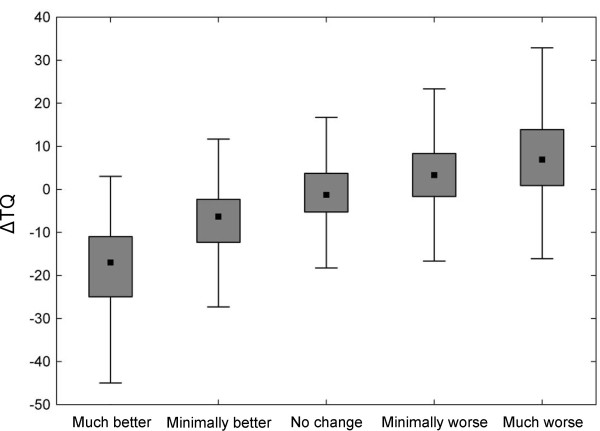
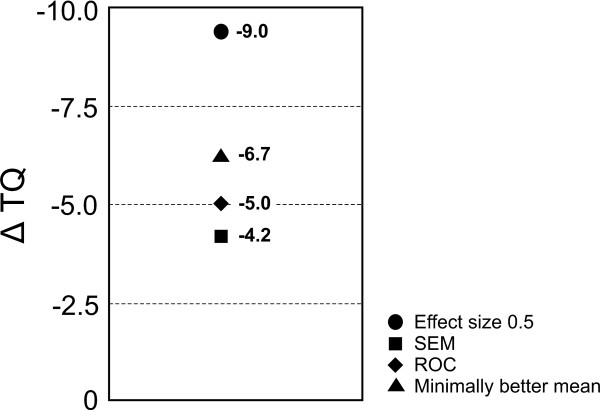
Results: The relationship between TQ change scores and CGI ratings of change was good (r = 0.52, p < 0.05). Mean change scores associated with minimally better and minimally worse CGI categories were -6.65 and +2.72 respectively. According to the ROC method MCID for improvement was -5 points and for deterioration +1 points.
Conclusion: Distribution and anchor-based methods yielded comparable results in identifying MCIDs. ΔTQ scores of -5 and +1 points were identified as the minimal clinically relevant change for improvement and worsening respectively. The asymmetry of the MCIDs for improvement and worsening may be related to expectation effects.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
