

The morphologic profile of HPV-related head and neck squamous carcinoma: implications for diagnosis, prognosis, and clinical management
- PMID: 22782223
- PMCID: PMC3394160
- DOI: 10.1007/s12105-012-0371-6
The morphologic profile of HPV-related head and neck squamous carcinoma: implications for diagnosis, prognosis, and clinical management
Abstract
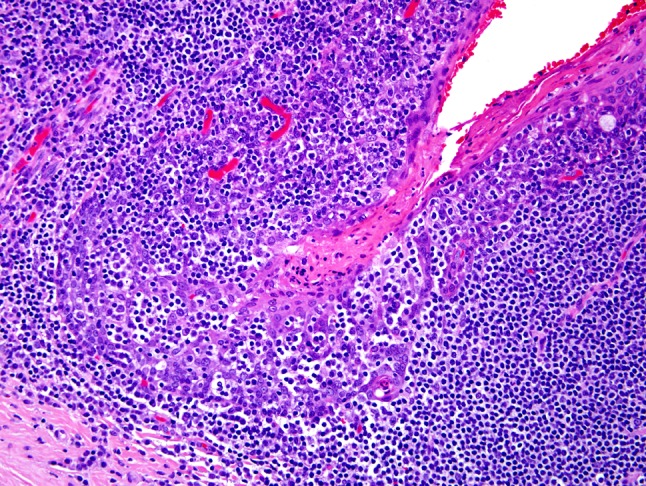
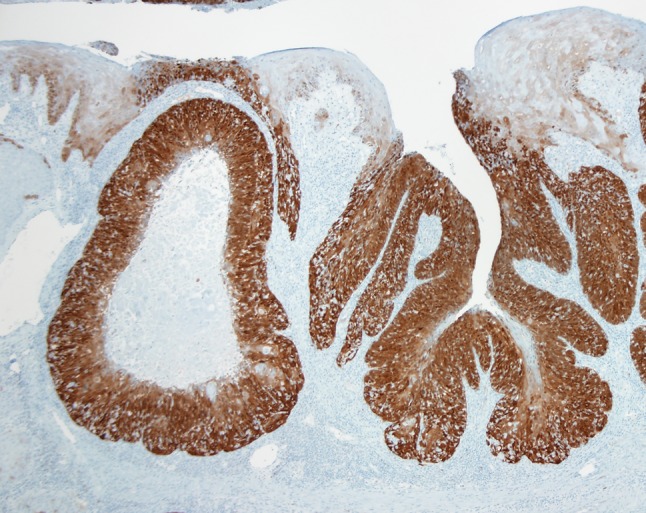
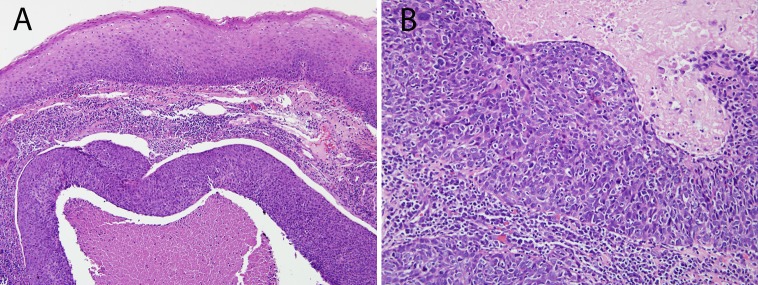
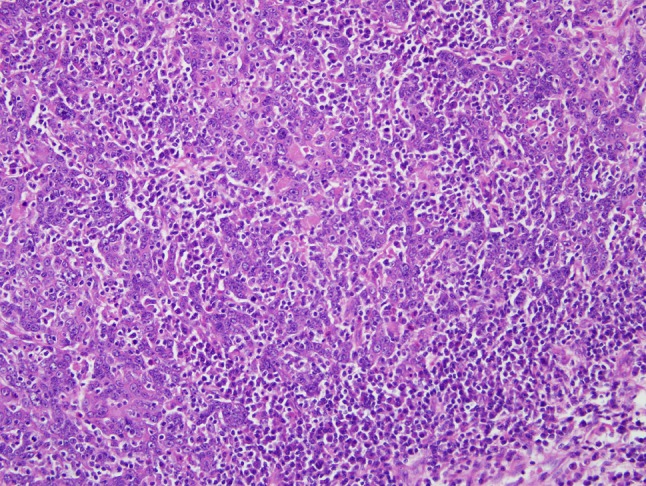
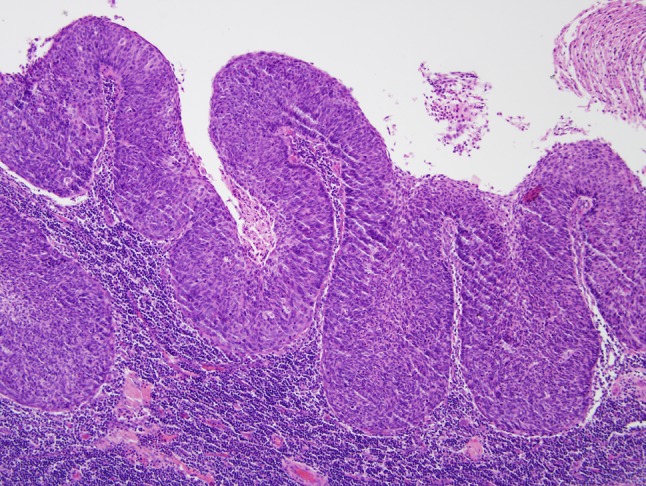
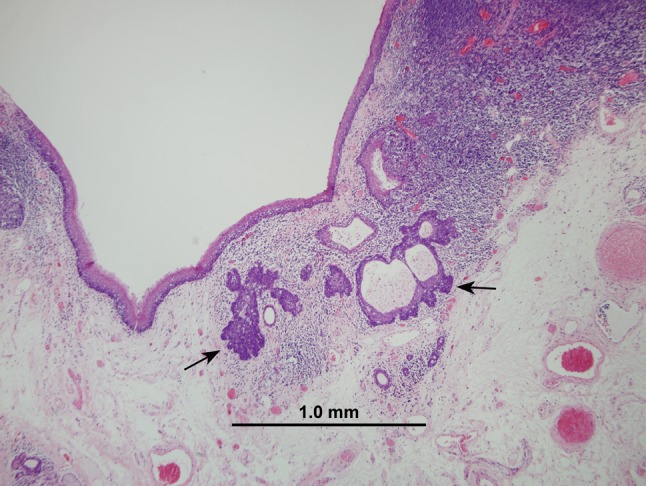
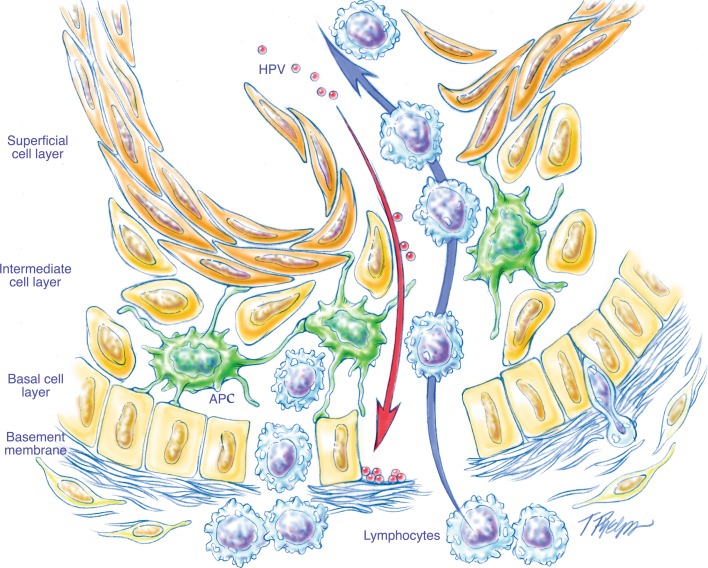
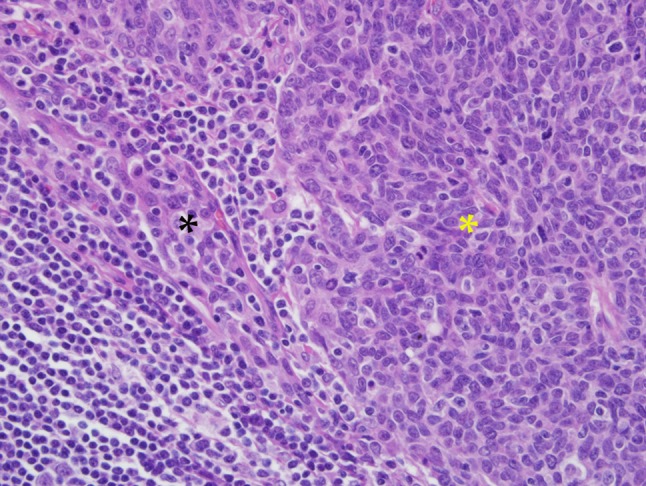
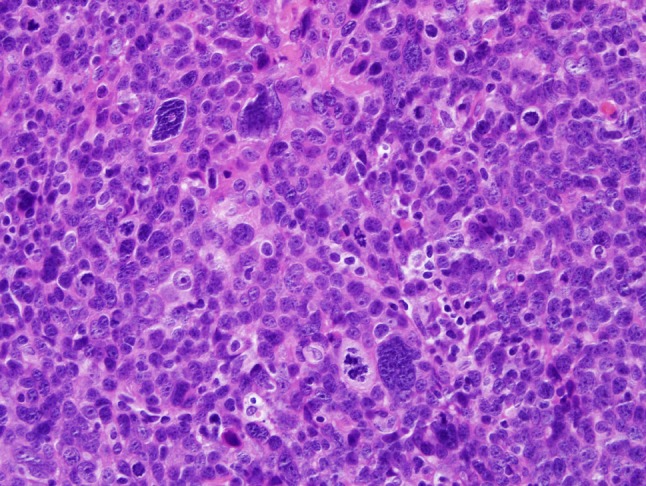
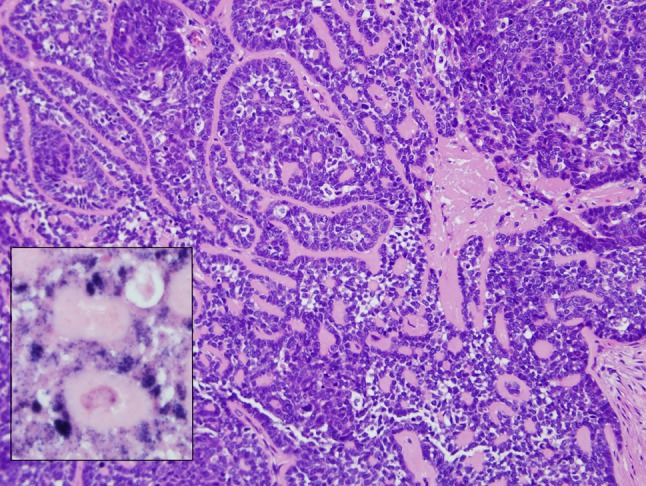
Much recent attention has highlighted a subset of head and neck squamous cell carcinomas (HNSCCs) related to the human papillomavirus (HPV) that is characterized by an epidemiologic, demographic, and clinical profile that deviates from the profile of conventional non-HPV-related HNSCC. Lost in the dash to develop and implement diagnostic assays to detect the presence of HPV in HNSCCs is the unpretentious observation that these HPV-HNSCCs are also distinctive with respect to their microscopic appearance, and that an awareness of these characteristic morphologic features can facilitate the diagnosis of HPV-related HNSCC (HPV-HNSCC). This review will delineate the microscopic appearance of HPV-HNSCC, spotlight ways in which the misinterpretation of these microscopic features can lead to diagnostic confusion, and provide recommendations for appropriate terminology when diagnosing HPV-HNSCC.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
