

Case Reports
doi: 10.1007/s10165-012-0715-9.
Epub 2012 Jul 11.
Clinical improvement in a patient with neuromyelitis optica following therapy with the anti-IL-6 receptor monoclonal antibody tocilizumab
Affiliations
- PMID: 22782533
- PMCID: PMC3713263
- DOI: 10.1007/s10165-012-0715-9
Item in Clipboard
Case Reports
Clinical improvement in a patient with neuromyelitis optica following therapy with the anti-IL-6 receptor monoclonal antibody tocilizumab
Mod Rheumatol.
2013 Jul.
Abstract
Neuromyelitis optica (NMO) is a disabling autoimmune disease associated with an elevation of anti-aquaporin 4 (AQP4) autoantibodies. Here, we present a case with NMO who responded to monthly administration of the anti-IL-6 receptor antibody tocilizumab. The treatment rapidly reduced the elevated numbers of plasmablasts and anti-AQP4 autoantibodies in the patient. Furthermore, neuropathic pain and disability scores gradually improved. Tocilizumab may be considered as a therapeutic option for NMO.
Figures
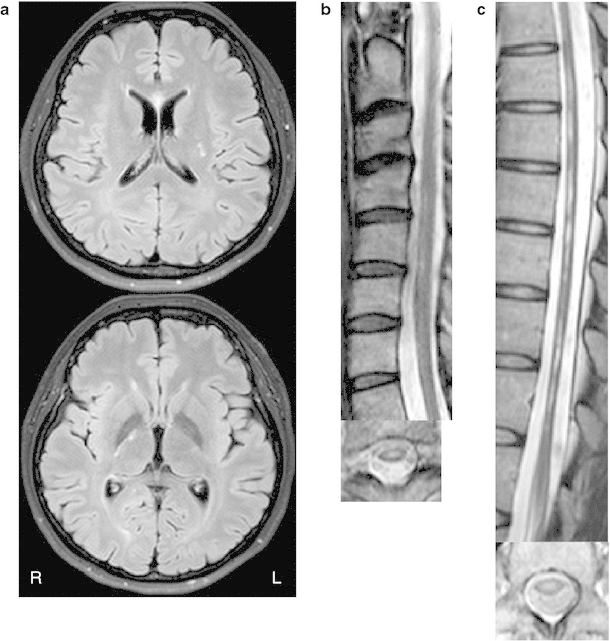
MRI before TCZ administration. a MRI showed multiple high-intensity lesions in the corpus callosum, left putamen, and right posterior limb of the internal capsule on T2-weighted images. b, c T2-weighted cervical and thoracic MRI demonstrates extensive scattered high-intensity lesions involving central gray matter
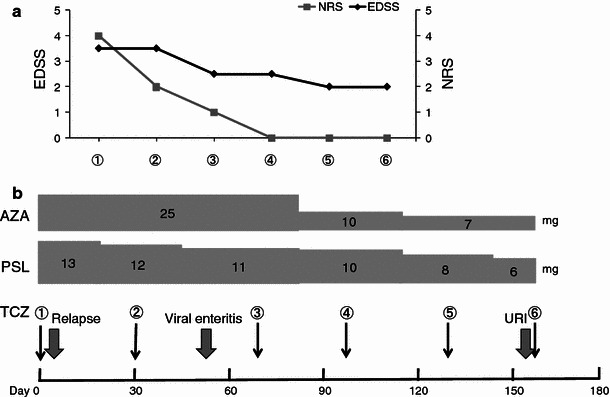
Clinical course after TCZ administration. a Follow-up for EDSS and NRS. b Dosages of concomitant drugs given to the patient (AZA and PSL). Numbers from 1–6 show the timing of each TCZ administration. URI upper respiratory infection
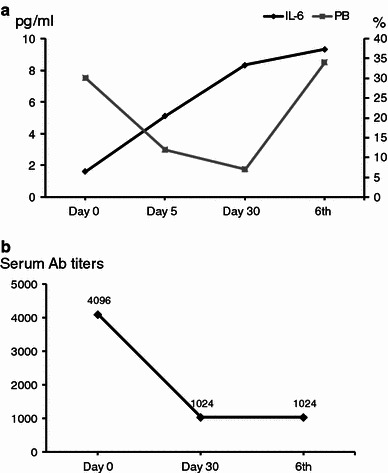
a Alterations in serum IL-6 and PB frequency (%) after injection of TCZ. Black dots and line represent the concentration of serum IL-6 (reference range: <4 pg/ml); gray dots and line represent the frequency of PB (%) among all B cells. Day 0 shortly before the first injection of TCZ, Day 5 five days after the first TCZ injection, Day 30 shortly before the second injection of TCZ, 6th shortly before the sixth TCZ injection. b Changes in the anti-AQP4 antibody titer
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
