

Left atrial structure and function and clinical outcomes in the general population
- PMID: 22782941
- PMCID: PMC3549524
- DOI: 10.1093/eurheartj/ehs188
Left atrial structure and function and clinical outcomes in the general population
Abstract
Aims: Left atrial (LA) structural and functional abnormalities may be subclinical phenotypes, which identify individuals at increased risk of adverse outcomes.
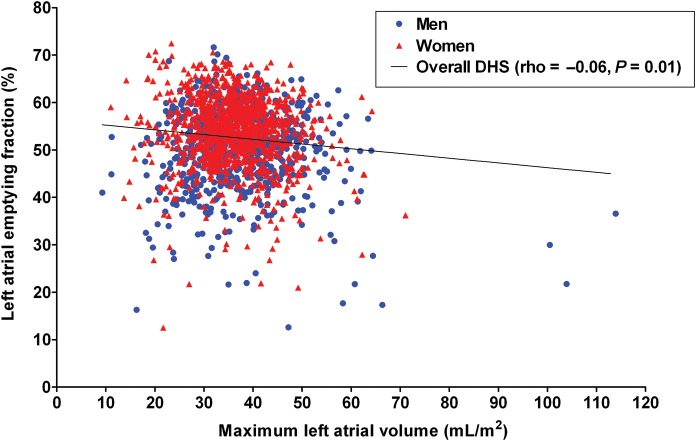
Methods and results: Maximum LA volume (LAmax) and LA emptying fraction (LAEF) were measured via cardiac magnetic resonance imaging in 1802 participants in the Dallas Heart Study. The associations of LAEF and LAmax indexed to body surface area (LAmax/BSA) with traditional risk factors, natriuretic peptide levels, and left ventricular (LV) structure [end-diastolic volume (EDV) and concentricity(0.67) (mass/EDV(0.67))] and function (ejection fraction) were assessed using linear regression analysis. The incremental prognostic value of LAmax/BSA and LAEF beyond traditional risk factors, LV ejection fraction, and LV mass was assessed using the Cox proportional-hazards model. Both increasing LAmax/BSA and decreasing LAEF were associated with hypertension and natriuretic peptide levels (P < 0.05 for all). In multivariable analysis, LAmax/BSA was most strongly associated with LV end-diastolic volume/BSA, while LAEF was strongly associated with LV ejection fraction and concentricity(0.67). During a median follow-up period of 8.1 years, there were 81 total deaths. Decreasing LAEF [hazard ratio (HR) per 1 standard deviation (SD) (8.0%): 1.56 (1.32-1.87)] but not increasing LAmax/BSA [HR per 1 SD (8.6 mL/m(2)): 1.14 (0.97-1.34)] was independently associated with mortality. Furthermore, the addition of LAEF to a model adjusting Framingham risk score, diabetes, race, LV mass, and ejection fraction improved the c-statistic (c-statistics: 0.78 vs. 0.77; P < 0.05, respectively), whereas the addition of LAmax/BSA did not (c-statistics: 0.76, P = 0.20).
Conclusion: In the general population, both LAmax/BSA and LAEF are important subclinical phenotypes but LAEF is superior and incremental to LAmax/BSA.
Figures



Comment in
-
What is the atrium trying to tell us?Eur Heart J. 2013 Jan;34(4):255-7. doi: 10.1093/eurheartj/ehs327. Epub 2012 Oct 22. Eur Heart J. 2013. PMID: 23091200 No abstract available.
References
-
- Wang TJ, Evans JC, Benjamin EJ, Levy D, LeRoy EC, Vasan RS. Natural history of asymptomatic left ventricular systolic dysfunction in the community. Circulation. 2003;108:977–982. - PubMed
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990;322:1561–1566. - PubMed
-
- Pritchett AM, Mahoney DW, Jacobsen SJ, Rodeheffer RJ, Karon BL, Redfield MM. Diastolic dysfunction and left atrial volume: a population-based study. J Am Coll Cardiol. 2005;45:87–92. - PubMed
-
- Gerdts E, Oikarinen L, Palmieri V, Otterstad JE, Wachtell K, Boman K, Dahlof B, Devereux RB. Correlates of left atrial size in hypertensive patients with left ventricular hypertrophy: the Losartan Intervention For Endpoint Reduction in Hypertension (LIFE) Study. Hypertension. 2002;39:739–743. - PubMed
-
- Gottdiener JS, Kitzman DW, Aurigemma GP, Arnold AM, Manolio TA. Left atrial volume, geometry, and function in systolic and diastolic heart failure of persons > or = 65 years of age (the Cardiovascular Health Study) Am J Cardiol. 2006;97:83–89. - PubMed
