

Relationship between 25-OH-D serum level and relapse rate in multiple sclerosis patients before and after vitamin D supplementation
- PMID: 22783368
- PMCID: PMC3388527
- DOI: 10.1177/1756285612447090
Relationship between 25-OH-D serum level and relapse rate in multiple sclerosis patients before and after vitamin D supplementation
Abstract
Background: Vitamin D could play a protective role in multiple sclerosis.
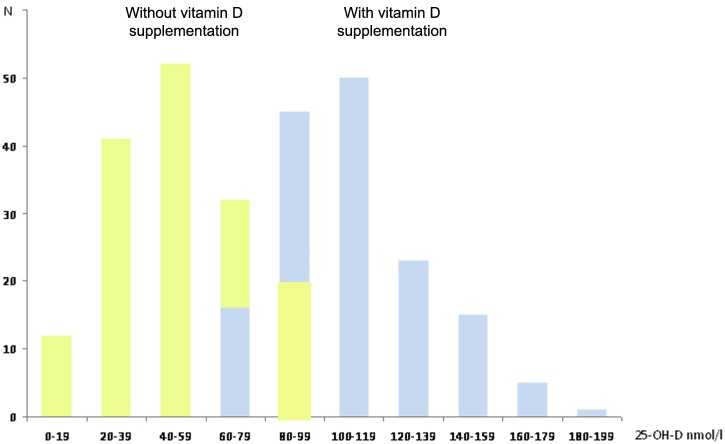
Methods: In an observational, uncontrolled study, vitamin D3 supplementation (3010 IU/day on average) was given to 156 consecutive patients with relapsing-remitting multiple sclerosis, under first-line immunomodulatory therapy and with initial 25-OH-D serum level lower than 100 nmol/l (40 ng/ml). Relapses were determined for 29.1 ± 8.4 months during vitamin D and 29.8 ± 10.1 months before supplementation. The 25-OH-D level was measured before supplementation and several times during supplementation. The incidence rate of relapses before and during supplementation was estimated using negative binomial regression models with follow-up durations as offset terms. The incidence rate and incidence rate ratio of relapses at various 25-OH-D levels were also calculated using negative binomial regression models.
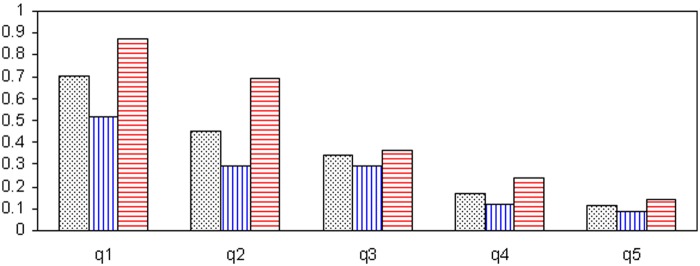
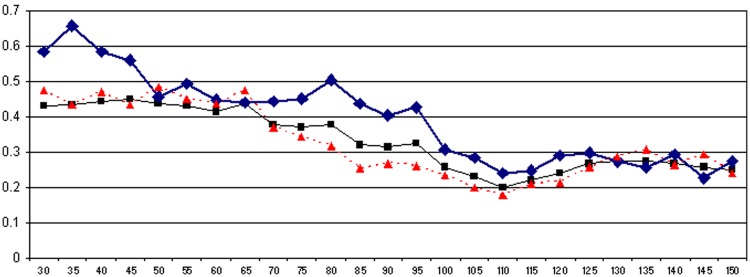
Results: In 76 patients, immunomodulatory therapy preceded vitamin D supplementation (by 4.2 ± 2.7 years) and in 80 patients both treatments were started simultaneously. Under supplementation, the 25-OH-D level increased from 49 ± 22 nmol/l to 110 ± 26 nmol/l on average. Pooling data collected before and during supplementation, we found a significant strong inverse relationship between the relapse incidence rate and the 25-OH-D level (p < 0.0001), suggesting that vitamin D did indeed influence the relapse rate. Results of univariate, bivariate and multivariate analyses were analogous: in the multivariate model adjusted for age, disease duration and previous use of immunomodulatory therapy, every 10 nmol increase in 25-OH-D level was associated with a reduction in the relapse incidence rate of 13.7%. Dividing iteratively the population made up of pooled periods into two subgroups according to the 25-OH-D levels, the relapse incidence rate ratio decreased as the 25-OH-D level increased up to 110 nmol/l, but a plateau effect was observed beyond this limit.
Conclusion: Further studies are warranted for accurate quantification of the vitamin D effect.
Keywords: multiple sclerosis; relapse rate; vitamin D; vitamin D supplementation.
Conflict of interest statement
Figures
References
-
- Ascherio A., Munger K.L. (2007) Environmental risk factors for multiple sclerosis. Part II: non-infectious factors. Ann Neurol 61: 504–513 - PubMed
-
- Ascherio A., Munger K.L., Simon K.C. (2010) Vitamin D and multiple sclerosis. Lancet Neurol 9: 599–612 - PubMed
-
- Bartosik-Psujek H., Tabarkiewicz J., Pocisnska K., Stelmasiak Z., Rolinski J. (2010) Immunomodulatory effects of vitamin D on monocyte-derived dendritic cells in multiple sclerosis. Mult Scler 16: 1513–1516 - PubMed
-
- Binkley N., Krueger D. (2008) Evaluation and correction of low vitamin D status. Curr Osteoporos Rep 6: 95-99 - PubMed
-
- Bischoff-Ferrari H.A., Giovannucci E., Willett W.C., Dietrich T., Dawson-Hughes B. (2006) Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 84: 18–28 - PubMed
LinkOut - more resources
Full Text Sources
