

Fertility-sparing treatment using medroxyprogesterone acetate for endometrial carcinoma
- PMID: 22783380
- PMCID: PMC3389624
- DOI: 10.3892/ol.2012.602
Fertility-sparing treatment using medroxyprogesterone acetate for endometrial carcinoma
Abstract
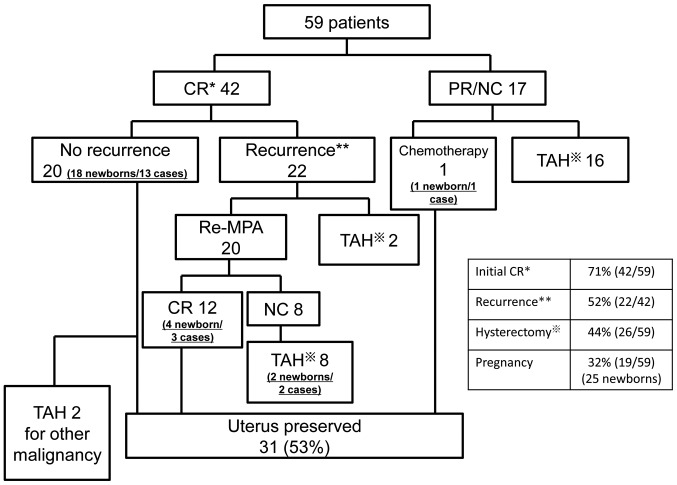
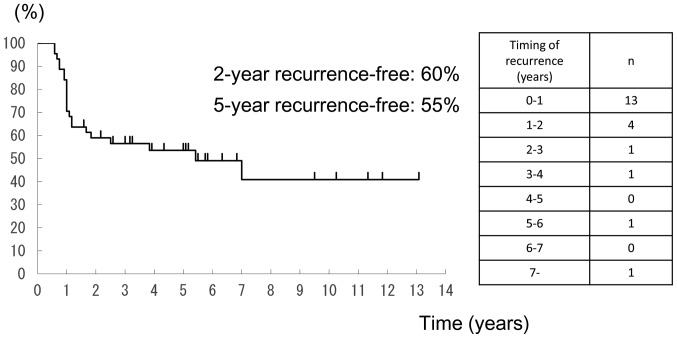
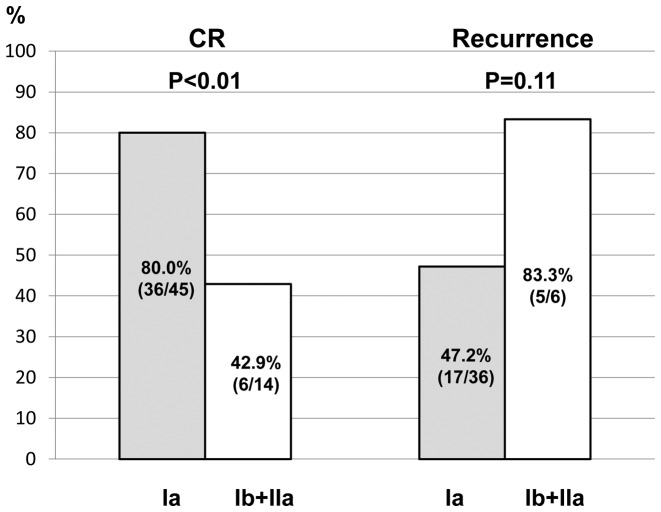
The purpose of this study was to present the results of fertility-sparing treatment using medroxyprogesterone acetate (MPA) for endometrial carcinoma (EC), and to clarify patient characteristics by investigating patient background factors. A total of 59 patients with EC, who received MPA as fertility-sparing therapy at two institutions over a 21-year period between 1987 and 2008, were studied retrospectively. Patients were administered oral MPA at 400-600 mg/day for 16-24 weeks as long as they responded. Endometrial tissue was assessed twice, at 8-12 weeks (during treatment) and shortly after treatment. The overall complete response (CR) rate was 71%. A total of 22 (52%) of 42 responders later developed relapse. A total of 19 cases became pregnant, and 25 infants were born. Eighty percent of recurrences occurred within 2 years. For stages I a and I b- II a (FIGO, 1988), initial CR rates were 80.0 and 42.9%, respectively (p<0.01), demonstrating a significant difference. Total hysterectomy was performed for 26 patients (44%) due to recurrence or failure to respond to the initial treatment. Among these 26 patients, postoperative stages were more advanced in 10 patients (38%). The grade advanced (became more poorly differentiated) postoperatively in 2 patients (8%). Premenopausal females with EC can be treated successfully with MPA, however patients should be informed of the risks and limitations of this conservative treatment.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Amant F, Moerman P, Neven P, Timmerman D, Van Limbergen E, Vergote I. Endometrial cancer. Lancet. 2005;366:491–505. - PubMed
-
- Parazzini F, La Vecchia C, Bocciolone L, Franceschi S. The epidemiology of endometrial cancer. Gynecol Oncol. 1991;41:1–16. - PubMed
-
- Brinton LA, Berman ML, Mortel R, et al. Reproductive, menstrual, and medical risk factors for endometrial cancer: results from a case-control study. Am J Obstet Gynecol. 1992;167:1317–1325. - PubMed
-
- Lurain JR. Uterine Cancer. In: Berek JS, editor. Berek & Novak’s Gynecology. 14th edition. Lippincott Williams & Wilkins; Philadelphia: 2007. pp. 1343–1401.
LinkOut - more resources
Full Text Sources