

Antiretroviral prophylaxis for HIV prevention in heterosexual men and women
- PMID: 22784037
- PMCID: PMC3770474
- DOI: 10.1056/NEJMoa1108524
Antiretroviral prophylaxis for HIV prevention in heterosexual men and women
Abstract
Background: Antiretroviral preexposure prophylaxis is a promising approach for preventing human immunodeficiency virus type 1 (HIV-1) infection in heterosexual populations.
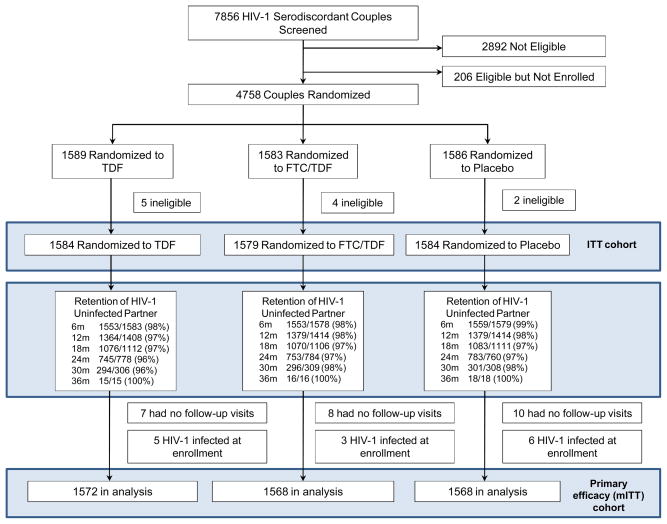
Methods: We conducted a randomized trial of oral antiretroviral therapy for use as preexposure prophylaxis among HIV-1-serodiscordant heterosexual couples from Kenya and Uganda. The HIV-1-seronegative partner in each couple was randomly assigned to one of three study regimens--once-daily tenofovir (TDF), combination tenofovir-emtricitabine (TDF-FTC), or matching placebo--and followed monthly for up to 36 months. At enrollment, the HIV-1-seropositive partners were not eligible for antiretroviral therapy, according to national guidelines. All couples received standard HIV-1 treatment and prevention services.
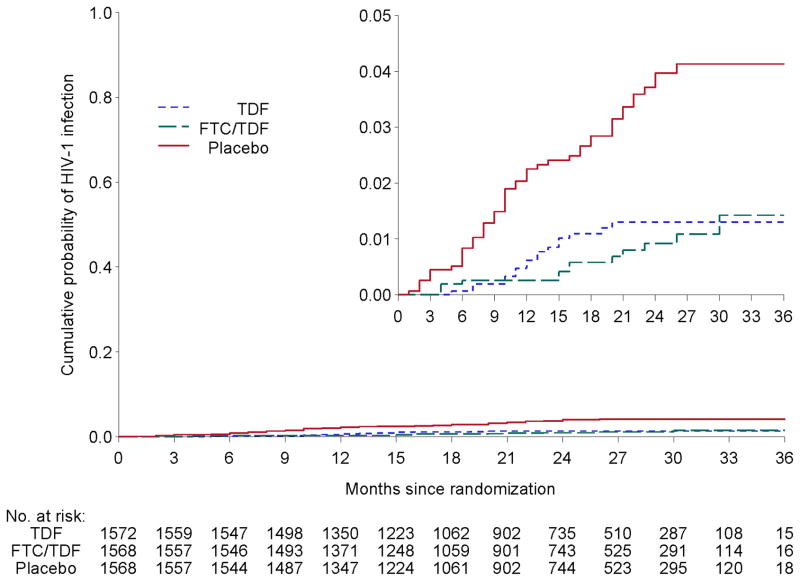
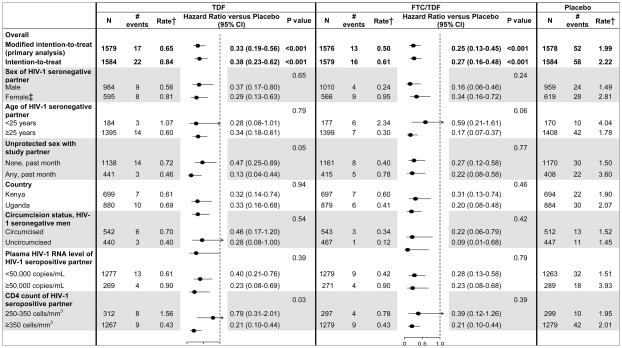
Results: We enrolled 4758 couples, of whom 4747 were followed: 1584 randomly assigned to TDF, 1579 to TDF-FTC, and 1584 to placebo. For 62% of the couples followed, the HIV-1-seronegative partner was male. Among HIV-1-seropositive participants, the median CD4 count was 495 cells per cubic millimeter (interquartile range, 375 to 662). A total of 82 HIV-1 infections occurred in seronegative participants during the study, 17 in the TDF group (incidence, 0.65 per 100 person-years), 13 in the TDF-FTC group (incidence, 0.50 per 100 person-years), and 52 in the placebo group (incidence, 1.99 per 100 person-years), indicating a relative reduction of 67% in the incidence of HIV-1 with TDF (95% confidence interval [CI], 44 to 81; P<0.001) and of 75% with TDF-FTC (95% CI, 55 to 87; P<0.001). Protective effects of TDF-FTC and TDF alone against HIV-1 were not significantly different (P=0.23), and both study medications significantly reduced the HIV-1 incidence among both men and women. The rate of serious adverse events was similar across the study groups. Eight participants receiving active treatment were found to have been infected with HIV-1 at baseline, and among these eight, antiretroviral resistance developed in two during the study.
Conclusions: Oral TDF and TDF-FTC both protect against HIV-1 infection in heterosexual men and women. (Funded by the Bill and Melinda Gates Foundation; Partners PrEP ClinicalTrials.gov number, NCT00557245.).
Figures
Comment in
-
Preexposure prophylaxis for HIV--where do we go from here?N Engl J Med. 2012 Aug 2;367(5):459-61. doi: 10.1056/NEJMe1207438. Epub 2012 Jul 11. N Engl J Med. 2012. PMID: 22784041 No abstract available.
-
ACP Journal Club. Preexposure prophylaxis reduced HIV-1 spread in serodiscordant heterosexual couples.Ann Intern Med. 2012 Nov 20;157(10):JC5-3. doi: 10.7326/0003-4819-157-10-201211200-02003. Ann Intern Med. 2012. PMID: 23165679 No abstract available.
-
Antiretroviral preexposure prophylaxis for HIV prevention.N Engl J Med. 2013 Jan 3;368(1):82. doi: 10.1056/NEJMc1210464. N Engl J Med. 2013. PMID: 23281987 No abstract available.
-
Antiretroviral preexposure prophylaxis for HIV prevention.N Engl J Med. 2013 Jan 3;368(1):83-4. doi: 10.1056/NEJMc1210464. N Engl J Med. 2013. PMID: 23293791 No abstract available.
-
Prophylactic antiretroviral HIV therapy prevents infection in heterosexual men and women.Evid Based Med. 2013 Oct;18(5):184-5. doi: 10.1136/eb-2012-101034. Epub 2013 Jan 24. Evid Based Med. 2013. PMID: 23349215 No abstract available.
-
Update in general internal medicine: evidence published in 2012.Ann Intern Med. 2013 Apr 16;158(8):615-9. doi: 10.7326/0003-4819-158-8-201304160-00101. Ann Intern Med. 2013. PMID: 23579948 No abstract available.
References
-
- Cohen MS, Gay C, Kashuba AD, Blower S, Paxton L. Narrative review: antiretroviral therapy to prevent the sexual transmission of HIV-1. Ann of Intern Med. 2007;146:591–601. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous