

Review
doi: 10.1056/NEJMra1202561.
Management of opioid analgesic overdose
Affiliations
- PMID: 22784117
- PMCID: PMC3739053
- DOI: 10.1056/NEJMra1202561
Item in Clipboard
Review
Management of opioid analgesic overdose
N Engl J Med.
.
No abstract available
Conflict of interest statement
Dr. Boyer reports reviewing medical malpractice documents for CRICO (Controlled Risk Insurance Company) Vermont, MCIC Vermont, and PMSLIC (Pennsylvania Medical Group Management Association). No other potential conflict of interest relevant to this article was reported.
Figures
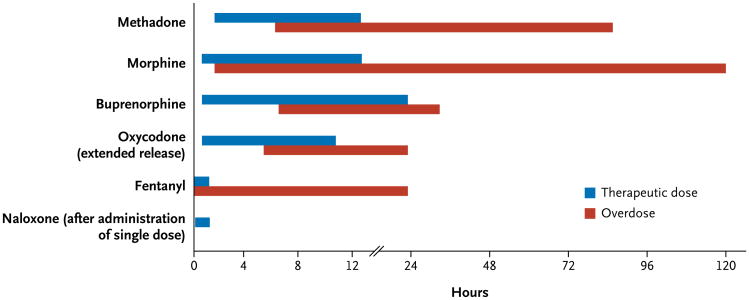
Information about the toxic effects of opioid analgesic overdose often must be synthesized from case reports, the clinical observations of medical toxicologists, and forensic data.- The difference between the clinical effects of therapeutic use and poisoning for these selected agents arises from the toxicokinetics of overdose, patterns of abuse, and the variation in drug effects in special populations.
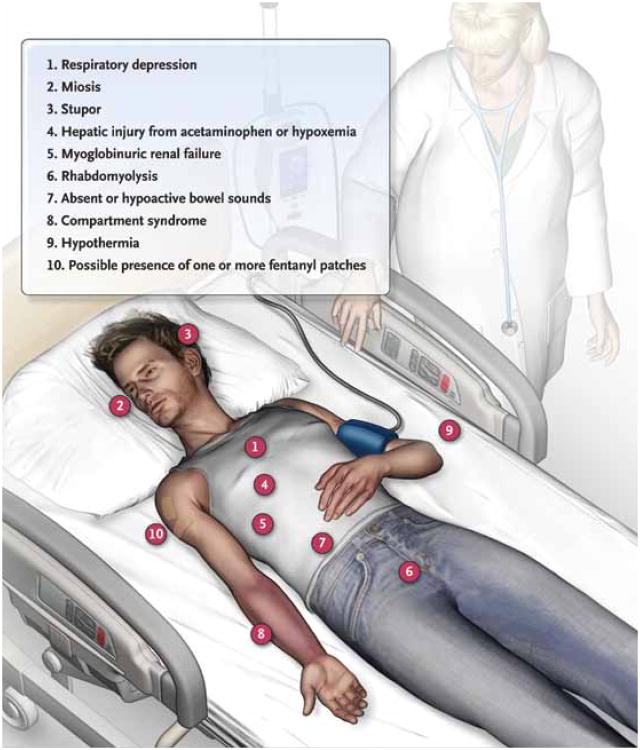
The sine qua non of opioid intoxication is respiratory depression, but miosis and stupor are often observed in poisoned patients. Hypoxemia or ingestion of drugs that are coformulated with acetaminophen can cause hepatic injury; acute renal failure can result from hypoxemia or precipitation of myoglobin due to rhabdomyolysis. Opioid analgesics decrease intestinal peristalsis by binding to opioid receptors in the gut. Patients with stupor who are motionless often have compressed fascia-bounded muscle groups, culminating in the compartment syndrome; they may also have hypothermia as a result of environmental exposure or misguided attempts at reversing intoxication. Since fentanyl can be a source of overdose, patients should be examined for the presence of fentanyl patches.
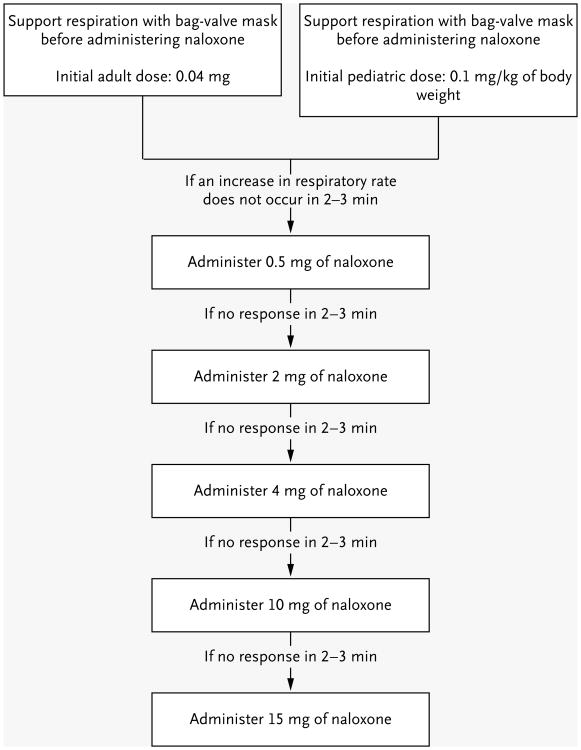
Empirical trials are needed to determine the effective dose of naloxone. Patients who do not have a response to an initial dose of naloxone should receive escalating doses until respiratory effort is restored. Naloxone, which is frequently dispensed as an injectable solution in doses of 0.4 mg per milliliter and 1 mg per milliliter for adults, is almost devoid of adverse effects. Pediatric patients are defined as children up to the age of about 5 years or with a body weight of up to 20 kg. Pediatric patients with opioid intoxication frequently require larger doses of naloxone to reverse the effects of overdose because of the relatively higher ingested dose per kilogram of body weight.
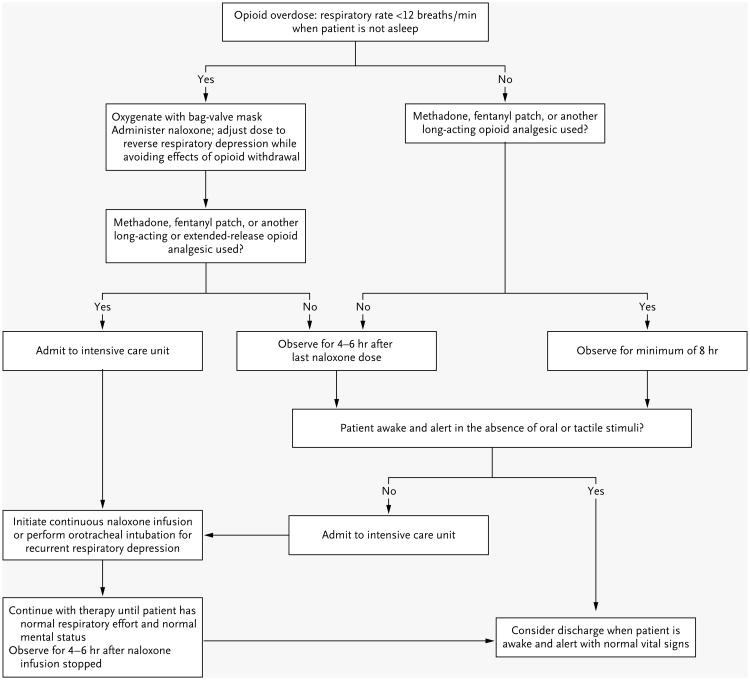
Because of the long duration of action of many opioid analgesic formulations, the brief effectiveness of naloxone, and the potential lethality of an opioid analgesic overdose, there should be a low threshold for admitting intoxicated patients to a hospital unit that provides close monitoring, such as an intensive care unit.,, Published guidelines for the management of opioid intoxication were developed on the basis of data from patients with heroin overdose and should not be applied to patients with opioid analgesic overdose.,
Comment in
-
Management of opioid analgesic overdose.N Engl J Med. 2012 Oct 4;367(14):1370-1; author reply 1372-3. doi: 10.1056/NEJMc1209707. N Engl J Med. 2012. PMID: 23034040 No abstract available.
-
Management of opioid analgesic overdose.N Engl J Med. 2012 Oct 4;367(14):1371; author reply 1372-3. doi: 10.1056/NEJMc1209707. N Engl J Med. 2012. PMID: 23034041 No abstract available.
-
Management of opioid analgesic overdose.N Engl J Med. 2012 Oct 4;367(14):1371-2; author reply 1372-3. doi: 10.1056/NEJMc1209707. N Engl J Med. 2012. PMID: 23034042 No abstract available.
-
Management of opioid analgesic overdose.N Engl J Med. 2012 Oct 4;367(14):1372; author reply 1372-3. doi: 10.1056/NEJMc1209707. N Engl J Med. 2012. PMID: 23034043 No abstract available.
References
-
- Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981–5. Erratum, N Engl J Med 2011;364:290. - PubMed
-
- Opioid analgesic risk evaluation and mitigation strategies (REMS): July 22-23, 2010 Joint Meeting of the Anesthetic and Life Support Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee. Silver Spring, MD: Food and Drug Administration; 2010.
-
- Allen L, Kimura K, MacKichan J, Ritschel W. Committee for Pharmacokinetic Nomenclature of the American College of Clinical Pharmacology. Manual of symbols, equations & definitions in pharmacokinetics. J Clin Pharmacol. 1982;22:1S–23S. - PubMed
-
- Larson AM, Polson J, Fontana RJ, et al. Acetaminophen-induced acute liver failure: results of a United States multicenter, prospective study. Hepatology. 2005;42:1364–72. - PubMed
-
- Paulozzi LJ, Budnitz D, Xi Y. Increasing deaths from opioid analgesics in the United States. Pharmacoepidemiol Drug Saf. 2006;15:618–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical