

Brief cognitive behavioral therapy in primary care: a hybrid type 2 patient-randomized effectiveness-implementation design
- PMID: 22784436
- PMCID: PMC3503767
- DOI: 10.1186/1748-5908-7-64
Brief cognitive behavioral therapy in primary care: a hybrid type 2 patient-randomized effectiveness-implementation design
Abstract
Background: Despite the availability of evidence-based psychotherapies for depression and anxiety, they are underused in non-mental health specialty settings such as primary care. Hybrid effectiveness-implementation designs have the potential to evaluate clinical and implementation outcomes of evidence-based psychotherapies to improve their translation into routine clinical care practices.
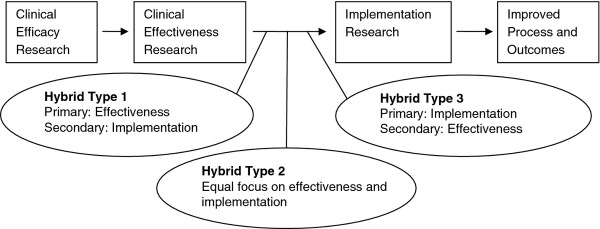
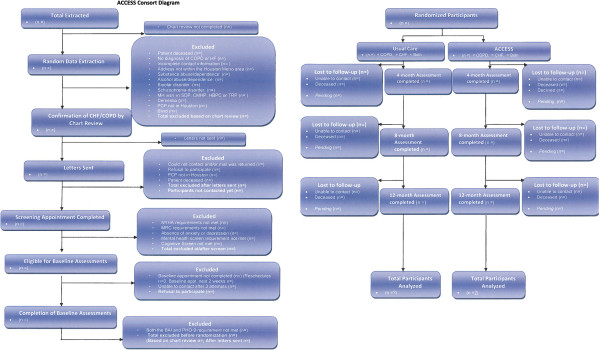
Methods: This protocol article discusses the study methodology and implementation strategies employed in an ongoing, hybrid, type 2 randomized controlled trial with two primary aims: (1) to determine whether a brief, manualized cognitive behavioral therapy administered by Veterans Affairs Primary Care Mental Health Integration program clinicians is effective in treating depression and anxiety in a sample of medically ill (chronic cardiopulmonary diseases) primary care patients and (2) to examine the acceptability, feasibility, and preliminary outcomes of a focused implementation strategy on improving adoption and fidelity of brief cognitive behavioral therapy at two Primary Care-Mental Health Integration clinics. The study uses a hybrid type 2 effectiveness/implementation design to simultaneously test clinical effectiveness and to collect pilot data on a multifaceted implementation strategy that includes an online training program, audit and feedback of session content, and internal and external facilitation. Additionally, the study engages the participation of an advisory council consisting of stakeholders from Primary Care-Mental Health Integration, as well as regional and national mental health leaders within the Veterans Administration. It targets recruitment of 320 participants randomized to brief cognitive behavioral therapy (n = 200) or usual care (n = 120). Both effectiveness and implementation outcomes are being assessed using mixed methods, including quantitative evaluation (e.g., intent-to-treat analyses across multiple time points) and qualitative methods (e.g., focus interviews and surveys from patients and providers). Patient-effectiveness outcomes include measures of depression, anxiety, and physical health functioning using blinded independent evaluators. Implementation outcomes include patient engagement and adherence and clinician brief cognitive behavioral therapy adoption and fidelity.
Conclusions: Hybrid designs are needed to advance clinical effectiveness and implementation knowledge to improve healthcare practices. The current article describes the rationale and challenges associated with the use of a hybrid design for the study of brief cognitive behavioral therapy in primary care. Although trade-offs exist between scientific control and external validity, hybrid designs are part of an emerging approach that has the potential to rapidly advance both science and practice.
Trial registration: NCT01149772 at http://www.clinicaltrials.gov/ct2/show/NCT01149772.
Figures
References
-
- Stanley MA, Beck JG, Novy DM, Averill PM, Swann AC, Diefenbach GJ. et al. Cognitive-behavioral treatment of late-life generalized anxiety disorder. J Consult Clin Psychol. 2003;71:309–319. Retrieved from PM:12699025. - PubMed
-
- Wenzel A, Brown GK, Karlin BE. Cognitive behavioral therapy for depression in veterans and military service members: therapist manual. Washington, D.C.: U.S. Department of Veterans Affairs; 2011.
-
- Whitfield G, Williams C. The evidence base for cognitive-behavioural therapy in depression: delivery in busy clinical settings. Adv Psychiatr Treat. 2003;9:21–30. doi: 10.1192/apt.9.1.21. Retrieved from http://apt.rcpsych.org/content/9/1/21.abstract. - DOI
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
