

Ultrasound-fluoroscopy registration for prostate brachytherapy dosimetry
- PMID: 22784870
- PMCID: PMC3448845
- DOI: 10.1016/j.media.2012.06.001
Ultrasound-fluoroscopy registration for prostate brachytherapy dosimetry
Abstract
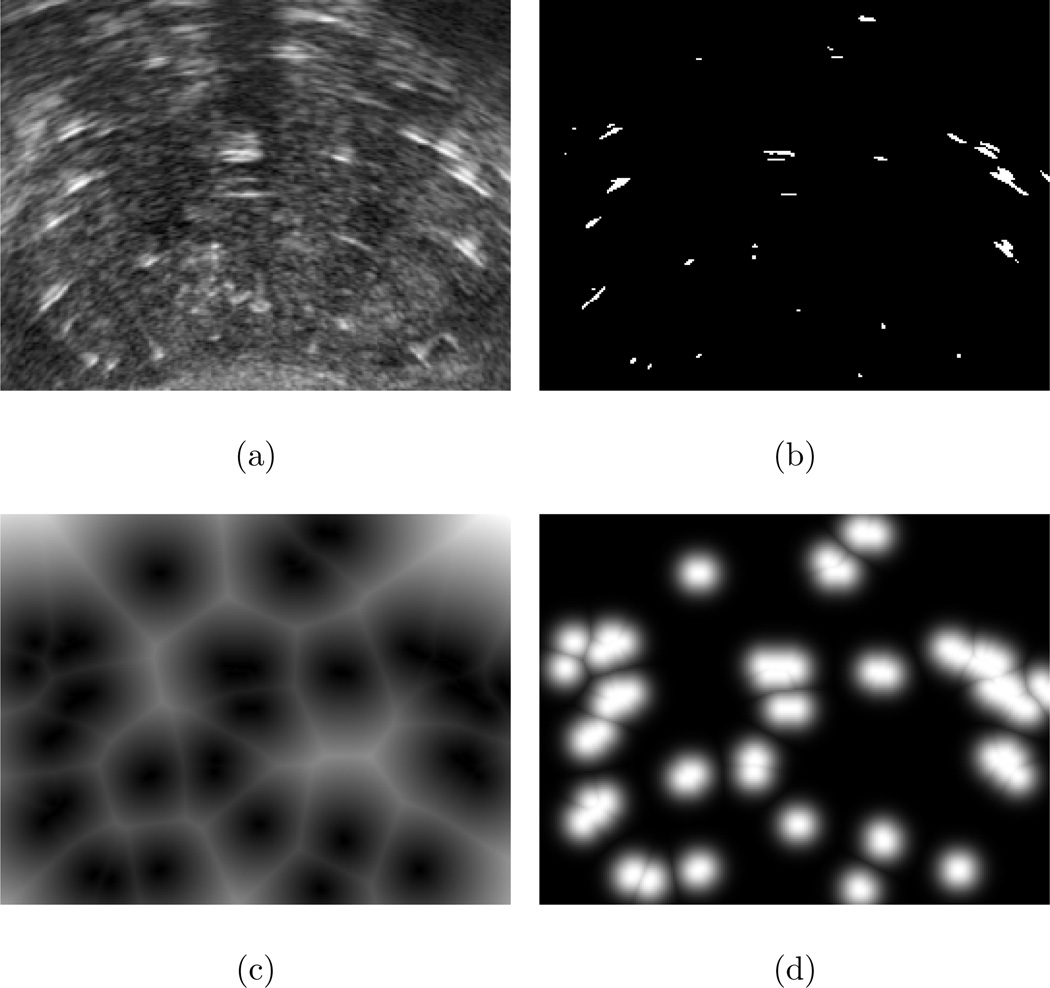
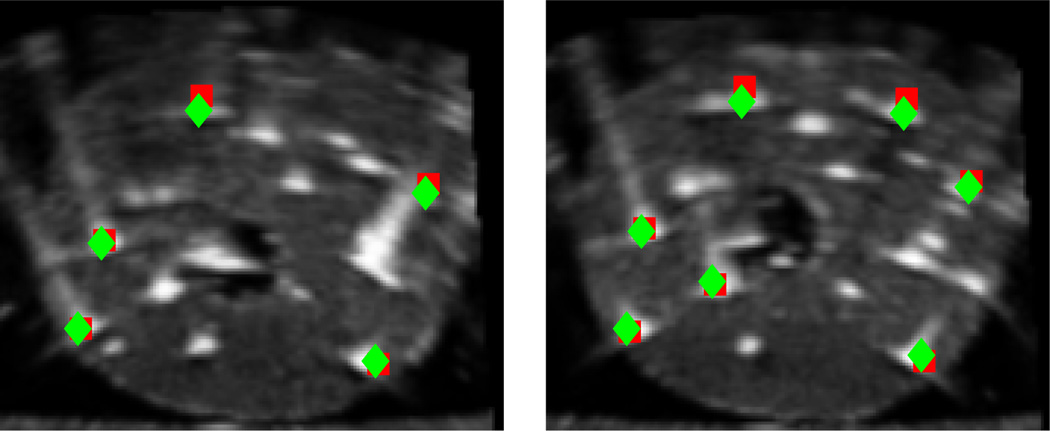
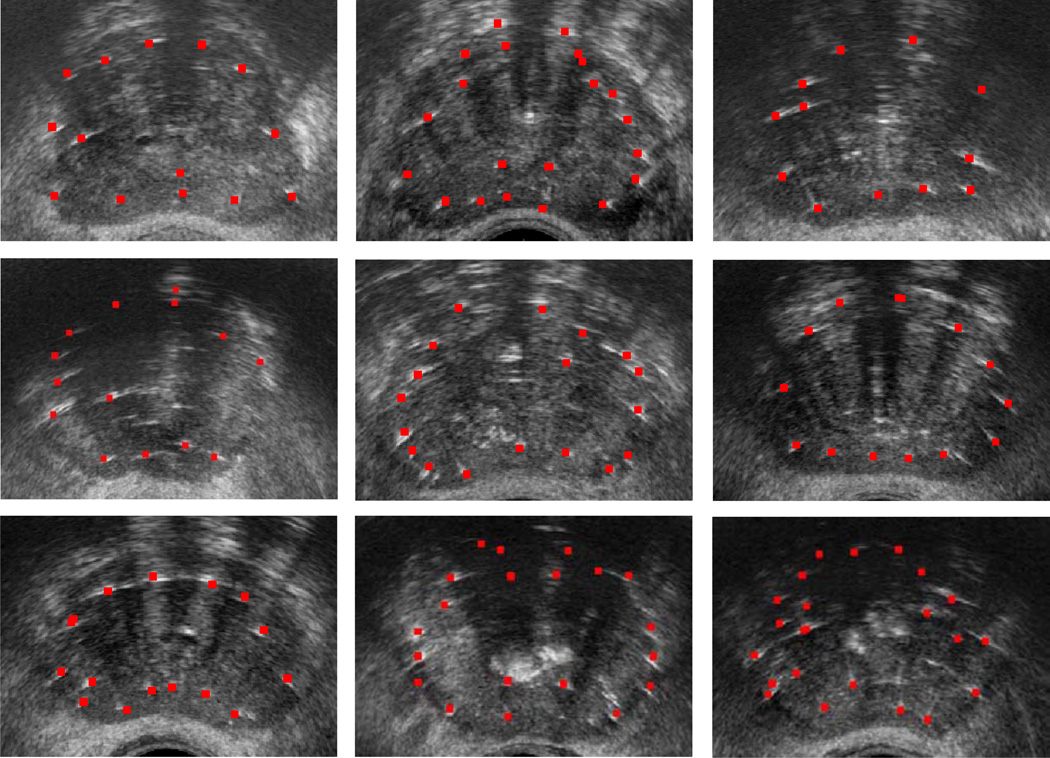
Prostate brachytherapy is a treatment for prostate cancer using radioactive seeds that are permanently implanted in the prostate. The treatment success depends on adequate coverage of the target gland with a therapeutic dose, while sparing the surrounding tissue. Since seed implantation is performed under transrectal ultrasound (TRUS) imaging, intraoperative localization of the seeds in ultrasound can provide physicians with dynamic dose assessment and plan modification. However, since all the seeds cannot be seen in the ultrasound images, registration between ultrasound and fluoroscopy is a practical solution for intraoperative dosimetry. In this manuscript, we introduce a new image-based nonrigid registration method that obviates the need for manual seed segmentation in TRUS images and compensates for the prostate displacement and deformation due to TRUS probe pressure. First, we filter the ultrasound images for subsequent registration using thresholding and Gaussian blurring. Second, a computationally efficient point-to-volume similarity metric, an affine transformation and an evolutionary optimizer are used in the registration loop. A phantom study showed final registration errors of 0.84 ± 0.45 mm compared to ground truth. In a study on data from 10 patients, the registration algorithm showed overall seed-to-seed errors of 1.7 ± 1.0 mm and 1.5 ± 0.9 mm for rigid and nonrigid registration methods, respectively, performed in approximately 30s per patient.
Copyright © 2012 Elsevier B.V. All rights reserved.
Figures


Similar articles
-
Registration between ultrasound and fluoroscopy or CT in prostate brachytherapy.Med Phys. 2010 Jun;37(6):2749-60. doi: 10.1118/1.3416937. Med Phys. 2010. PMID: 20632585
-
An image-guidance system for dynamic dose calculation in prostate brachytherapy using ultrasound and fluoroscopy.Med Phys. 2014 Sep;41(9):091712. doi: 10.1118/1.4893761. Med Phys. 2014. PMID: 25186387 Free PMC article.
-
Computing intraoperative dosimetry for prostate brachytherapy using TRUS and fluoroscopy.Acad Radiol. 2005 Oct;12(10):1262-72. doi: 10.1016/j.acra.2005.05.026. Acad Radiol. 2005. PMID: 16179203
-
EM-enhanced US-based seed detection for prostate brachytherapy.Med Phys. 2018 Jun;45(6):2357-2368. doi: 10.1002/mp.12894. Epub 2018 Apr 24. Med Phys. 2018. PMID: 29604086
-
Clinical evaluation of an MRI-to-ultrasound deformable image registration algorithm for prostate brachytherapy.Brachytherapy. 2019 Jan-Feb;18(1):95-102. doi: 10.1016/j.brachy.2018.08.006. Epub 2018 Oct 2. Brachytherapy. 2019. PMID: 30287271 Review.
Cited by
-
Deformable registration of X-ray to MRI for post-implant dosimetry in prostate brachytherapy.Proc SPIE Int Soc Opt Eng. 2016 Feb-Mar;9786:97860L. doi: 10.1117/12.2216911. Epub 2016 Mar 18. Proc SPIE Int Soc Opt Eng. 2016. PMID: 32419717 Free PMC article.
-
A Dynamic Dosimetry System for Prostate Brachytherapy.Proc SPIE Int Soc Opt Eng. 2013 Mar 8;8671:10.1117/12.2008097. doi: 10.1117/12.2008097. Proc SPIE Int Soc Opt Eng. 2013. PMID: 24392207 Free PMC article.
-
Intraoperative segmentation of iodine and palladium radioactive sources in C-arm images.Int J Comput Assist Radiol Surg. 2014 Sep;9(5):769-76. doi: 10.1007/s11548-014-0983-2. Epub 2014 Feb 7. Int J Comput Assist Radiol Surg. 2014. PMID: 24504857
-
Superior Postimplant Dosimetry Achieved Using Dynamic Intraoperative Dosimetry for Permanent Prostate Brachytherapy.Pract Radiat Oncol. 2021 Jul-Aug;11(4):264-271. doi: 10.1016/j.prro.2021.03.001. Epub 2021 Mar 13. Pract Radiat Oncol. 2021. PMID: 33722782 Free PMC article.
-
Intraoperative Registered Ultrasound and Fluoroscopy (iRUF) for dose calculation during prostate brachytherapy: Improved accuracy compared to standard ultrasound-based dosimetry.Radiother Oncol. 2017 Jul;124(1):61-67. doi: 10.1016/j.radonc.2017.05.018. Epub 2017 Jun 21. Radiother Oncol. 2017. PMID: 28647400 Free PMC article.
References
-
- Amols HI, Rosen II. A three-film technique for reconstruction of radioactive seed implants. Med. Phys. 1981;8(2):210–214. - PubMed
-
- Blasko JC, Mate T, Sylvester JE, Grimm PD, Cavanagh W. Brachytherapy for carcinoma of the prostate: Techniques, patient selection, and clinical outcomes. Semin. Radiat. Oncol. 2002;12(1):81–94. Advances in Brachytherapy. - PubMed
-
- Brunet-Benkhoucha M, Verhaegen F, Reniers B, Lassalle S, Béliveau-Nadeau D, Donath D, Taussky D, Carrier J-F. Clinical implementation of a digital tomosynthesis-based seed reconstruction algorithm for intraoperative postimplant dose evaluation in low dose rate prostate brachytherapy. Med. Phys. 2009;36(11):5235–5244. - PubMed
-
- Chen TK, Thurston AD, Ellis RE, Abolmaesumi P. A real-time freehand ultrasound calibration system with automatic accuracy feedback and control. Ultrasound Med. Biol. 2009;35(1):79–93. - PubMed
-
- Davis BJ, Horwitz EM, Lee WR, Crook JM, Stock RG, Merrick GS, Butler WM, Grimm PD, Stone NN, Potters L, Zietman AL, Zelefsky MJ. American brachytherapy society consensus guidelines for transrectal ultrasound-guided permanent prostate brachytherapy. Brachytherapy. 2012;11(1):6–19. - PubMed
