

Reirradiation of recurrent meningioma
- PMID: 22784877
- PMCID: PMC3884216
- DOI: 10.1016/j.jocn.2012.01.023
Reirradiation of recurrent meningioma
Abstract
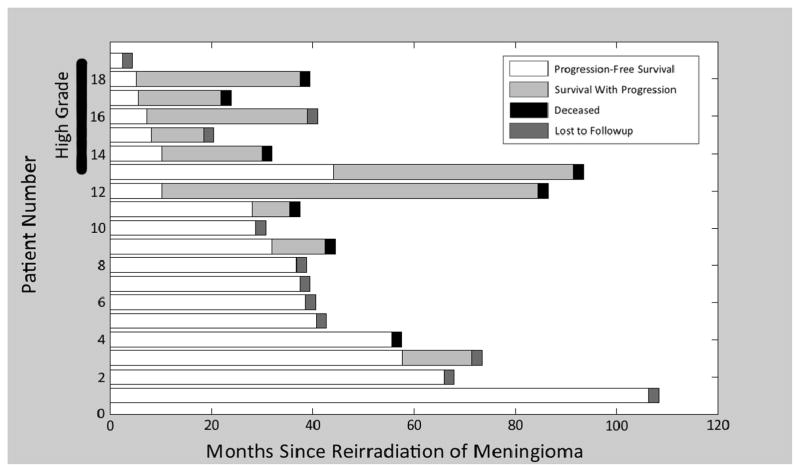
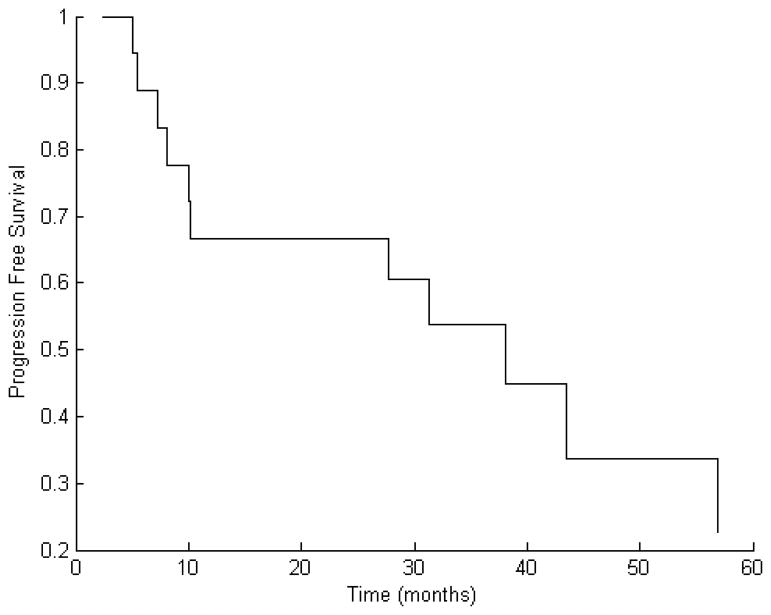
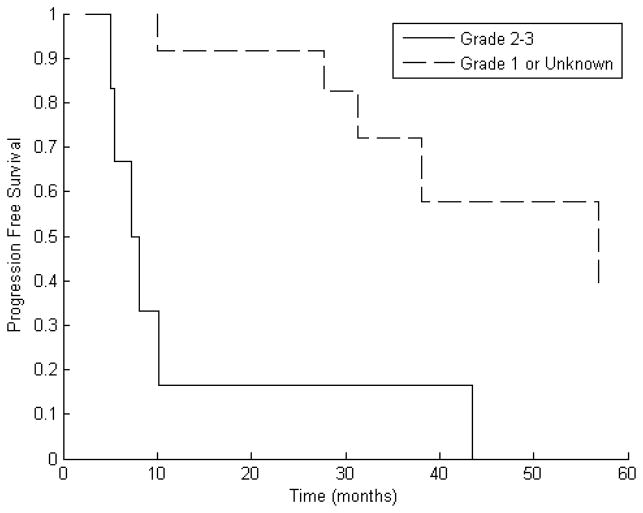
Management of meningioma includes observation, resection, and radiation therapy (RT). For patients with recurrent disease, similar options exist. However, the control rate following a second course of RT for recurrent disease is unknown. We reviewed an institutional database of patients with meningioma treated with stereotactic radiosurgery or fractionated stereotactic RT who underwent a second course for recurrent disease. Cox regression model was used for analysis. Variables tested included tumor volume, RT type, tumor grade, age at diagnosis, time to progression, and interval between RT. Eleven of 19 patients (58%) experienced disease progression. Median time to second progression was 10 months. Freedom from progression at one year was lower in patients with grade II or III tumors compared to those with grade 1 or unknown histology (17% compared to 92%, p=0.0054). Cox regression showed that a grade II-III tumor affects progression-free survival (PFS), with a hazard ratio of 5.37 (p=0.011). Median time to progression (MTP) for patients with grade II-III tumors was eight months. MTP was not reached for patients with grade 1/unknown tumors. Reirradiation for recurrent meningioma yields modest tumor control rates but for patients with grade II or III tumors, outcomes are poor.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Stereotactic radiotherapy as primary definitive or postoperative treatment of intracranial meningioma of WHO grade II and III leads to better disease control than stereotactic radiotherapy of recurrent meningioma.J Neurooncol. 2017 Sep;134(2):407-416. doi: 10.1007/s11060-017-2540-7. Epub 2017 Jun 30. J Neurooncol. 2017. PMID: 28667597
-
Radiologic Response and Disease Control of Recurrent Intracranial Meningiomas Treated With Reirradiation.Int J Radiat Oncol Biol Phys. 2018 Sep 1;102(1):194-203. doi: 10.1016/j.ijrobp.2018.05.011. Epub 2018 Jun 30. Int J Radiat Oncol Biol Phys. 2018. PMID: 29970312
-
Analysis of the results of recurrent intracranial meningiomas treated with re-radiosurgery.Clin Neurol Neurosurg. 2017 Feb;153:93-101. doi: 10.1016/j.clineuro.2016.12.014. Epub 2016 Dec 29. Clin Neurol Neurosurg. 2017. PMID: 28081463
-
Grade II meningiomas and Gamma Knife radiosurgery: analysis of success and failure to improve treatment paradigm.J Neurosurg. 2016 Dec;125(Suppl 1):89-96. doi: 10.3171/2016.7.GKS161521. J Neurosurg. 2016. PMID: 27903189
-
Stereotactic radiosurgery versus stereotactic radiotherapy in the management of intracranial meningiomas: a systematic review and meta-analysis.Neurosurg Focus. 2019 Jun 1;46(6):E2. doi: 10.3171/2019.3.FOCUS1970. Neurosurg Focus. 2019. PMID: 31153149
Cited by
-
Brachytherapy with surgical resection as salvage treatment for recurrent high-grade meningiomas: a matched cohort study.J Neurooncol. 2020 Jan;146(1):111-120. doi: 10.1007/s11060-019-03342-5. Epub 2019 Nov 19. J Neurooncol. 2020. PMID: 31745706
-
Evaluation of particle radiotherapy for the re-irradiation of recurrent intracranial meningioma.Radiat Oncol. 2018 May 8;13(1):86. doi: 10.1186/s13014-018-1026-x. Radiat Oncol. 2018. PMID: 29739417 Free PMC article.
-
Clinical Outcomes of Recurrent Intracranial Meningiomas Treated with Proton Beam Reirradiation.Int J Part Ther. 2019 Spring;5(4):11-22. doi: 10.14338/IJPT-18-00045.1. Epub 2019 May 1. Int J Part Ther. 2019. PMID: 31773037 Free PMC article.
-
Radiation therapy for atypical and anaplastic meningiomas: an overview of current results and controversial issues.Neurosurg Rev. 2022 Oct;45(5):3019-3033. doi: 10.1007/s10143-022-01806-3. Epub 2022 Jun 4. Neurosurg Rev. 2022. PMID: 35665867 Free PMC article. Review.
-
Management of Recurrent Meningiomas: State of the Art and Perspectives.Cancers (Basel). 2022 Aug 18;14(16):3995. doi: 10.3390/cancers14163995. Cancers (Basel). 2022. PMID: 36010988 Free PMC article. Review.
References
-
- Central Brain Tumor Registry of the United States; 2009. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2004–2005 [database on the Internet] Available from: http://www.cbtrus.org.
-
- Mirimanoff RDD, Linggood R, et al. Meningioma: analysis of recurrence and progression following neurosurgical resection. Journal of Neurosurgery. 1985;(62):18–24. - PubMed
-
- Davidson L, Fishback D, Russin JJ, et al. Postoperative Gamma Knife surgery for benign meningiomas of the cranial base. Neurosurg Focus. 2007;23(4):E6. - PubMed
-
- Miralbell R, Linggood RM, de la Monte S, et al. The role of radiotherapy in the treatment of subtotally resected benign meningiomas. J Neurooncol. 1992;13(2):157–64. - PubMed
-
- Taylor BW, Jr, Marcus RB, Jr, Friedman WA, et al. The meningioma controversy: postoperative radiation therapy. Int J Radiat Oncol Biol Phys. 1988;15(2):299–304. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
