

Preclinical modeling of EGFR inhibitor resistance in head and neck cancer
- PMID: 22785204
- PMCID: PMC3414414
- DOI: 10.4161/cbt.20846
Preclinical modeling of EGFR inhibitor resistance in head and neck cancer
Abstract
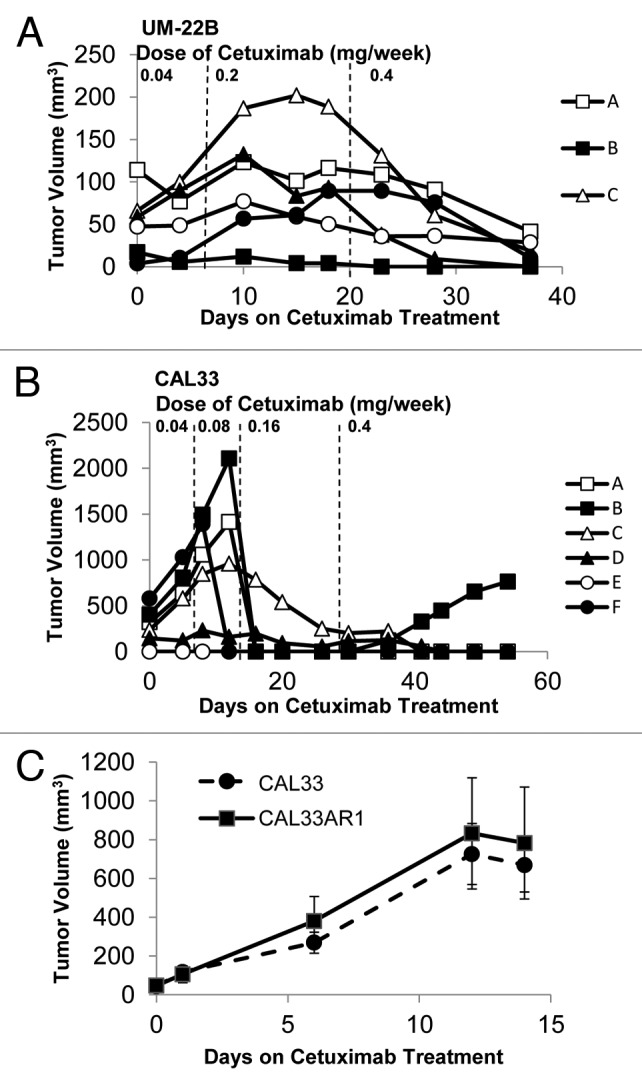
The epidermal growth factor receptor (EGFR) is widely expressed in head and neck squamous cell carcinomas (HNSCC) and can activate many growth and survival pathways within tumor cells. Despite ubiquitous EGFR expression, therapies targeting the receptor are only modestly effective in the treatment of HNSCC. A consistent mechanism of resistance to EGFR targeting agents has not yet been identified in HNSCC likely due, in part, to the paucity of preclinical models. We assessed the in vitro and in vivo responses of a panel of 10 genotypically validated HNSCC cell lines to the EGFR inhibitors erlotinib and cetuximab to determine their validity as models of resistance to these agents. We defined a narrow range of response to erlotinib in HNSCC cells in vitro and found a positive correlation between EGFR protein expression and erlotinib response. We observed cross-sensitivity in one HNSCC cell line, 686LN, between erlotinib and cetuximab in vivo. We attempted to generate models of cetuximab resistance in HNSCC cell line-derived xenografts and heterotopic tumorgrafts generated directly from primary patient tumors. While all 10 HNSCC cell line xenografts tested were sensitive to cetuximab in vivo, heterotopic patient tumorgrafts varied in response to cetuximab indicating that these models may be more representative of clinical responses. These studies demonstrate the limitations of using HNSCC cell lines to reflect the heterogeneous clinical responses to erlotinib and cetuximab, and suggest that different approaches including heterotopic tumorgrafts may prove more valuable to elucidate mechanisms of clinical resistance to EGFR inhibitors in HNSCC.
Figures




Similar articles
-
Targeting Stat3 abrogates EGFR inhibitor resistance in cancer.Clin Cancer Res. 2012 Sep 15;18(18):4986-96. doi: 10.1158/1078-0432.CCR-12-0792. Epub 2012 Jul 23. Clin Cancer Res. 2012. PMID: 22825581 Free PMC article.
-
Honokiol inhibits epidermal growth factor receptor signaling and enhances the antitumor effects of epidermal growth factor receptor inhibitors.Clin Cancer Res. 2010 May 1;16(9):2571-9. doi: 10.1158/1078-0432.CCR-10-0333. Epub 2010 Apr 13. Clin Cancer Res. 2010. PMID: 20388852 Free PMC article.
-
MyD88-Dependent Signaling Decreases the Antitumor Efficacy of Epidermal Growth Factor Receptor Inhibition in Head and Neck Cancer Cells.Cancer Res. 2015 Apr 15;75(8):1657-67. doi: 10.1158/0008-5472.CAN-14-2061. Epub 2015 Feb 20. Cancer Res. 2015. PMID: 25712126 Free PMC article.
-
Epidermal growth factor receptor targeted therapy of squamous cell carcinoma of the head and neck.Head Neck. 2010 Oct;32(10):1412-21. doi: 10.1002/hed.21365. Head Neck. 2010. PMID: 20848399 Free PMC article. Review.
-
The role of cetuximab for the treatment of squamous cell carcinoma of the head and neck.Clin Adv Hematol Oncol. 2008 Oct;6(10):742-50. Clin Adv Hematol Oncol. 2008. PMID: 18997665 Free PMC article. Review.
Cited by
-
Establishment of head and neck squamous cell carcinoma mouse models for cetuximab resistance and sensitivity.Cancer Drug Resist. 2023 Oct 17;6(4):709-728. doi: 10.20517/cdr.2023.62. eCollection 2023. Cancer Drug Resist. 2023. PMID: 38239393 Free PMC article.
-
Constitutive or Induced HIF-2 Addiction is Involved in Resistance to Anti-EGFR Treatment and Radiation Therapy in HNSCC.Cancers (Basel). 2019 Oct 21;11(10):1607. doi: 10.3390/cancers11101607. Cancers (Basel). 2019. PMID: 31640284 Free PMC article.
-
Inhibition of EphB4-Ephrin-B2 Signaling Enhances Response to Cetuximab-Radiation Therapy in Head and Neck Cancers.Clin Cancer Res. 2018 Sep 15;24(18):4539-4550. doi: 10.1158/1078-0432.CCR-18-0327. Epub 2018 May 30. Clin Cancer Res. 2018. PMID: 29848571 Free PMC article.
-
Targeting secondary immune responses to cetuximab: CD137 and the outside story.J Clin Invest. 2014 Jun;124(6):2371-5. doi: 10.1172/JCI76264. Epub 2014 May 16. J Clin Invest. 2014. PMID: 24837438 Free PMC article.
-
Therapeutic potential for P2Y2 receptor antagonism.Purinergic Signal. 2023 Jun;19(2):401-420. doi: 10.1007/s11302-022-09900-3. Epub 2022 Oct 11. Purinergic Signal. 2023. PMID: 36219327 Free PMC article. Review.
References
-
- Mrhalova M, Plzak J, Betka J, Kodet R. Epidermal growth factor receptor--its expression and copy numbers of EGFR gene in patients with head and neck squamous cell carcinomas. Neoplasma. 2005;52:338–43. - PubMed
-
- Grandis JR, Tweardy DJ. Elevated levels of transforming growth factor alpha and epidermal growth factor receptor messenger RNA are early markers of carcinogenesis in head and neck cancer. Cancer Res. 1993;53:3579–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous