

Risk of pneumonia associated with use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers: systematic review and meta-analysis
- PMID: 22786934
- PMCID: PMC3394697
- DOI: 10.1136/bmj.e4260
Risk of pneumonia associated with use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers: systematic review and meta-analysis
Abstract
Objective: To systematically review longitudinal studies evaluating use of angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) and risk of pneumonia.
Design: Systematic review and meta-analysis.
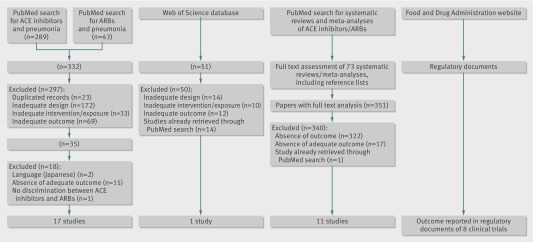
Data sources: Medline through PubMed, Web of Science with conference proceedings (inception to June 2011), and US Food and Drug Administration website (June 2011). Systematic reviews and references of retrieved articles were also searched.
Study selection: Two reviewers independently selected randomised controlled trials and cohort and case-control studies evaluating the use of ACE inhibitors or ARBs and risk of pneumonia and retrieved characteristics of the studies and data estimates.
Data synthesis: The primary outcome was incidence of pneumonia and the secondary outcome was pneumonia related mortality. Subgroup analyses were carried according to baseline morbidities (stroke, heart failure, and chronic kidney disease) and patients' characteristics (Asian and non-Asian). Pooled estimates of odds ratios and 95% confidence intervals were derived by random effects meta-analysis. Adjusted frequentist indirect comparisons between ACE inhibitors and ARBs were estimated and combined with direct evidence whenever available. Heterogeneity was assessed using the I(2) test.
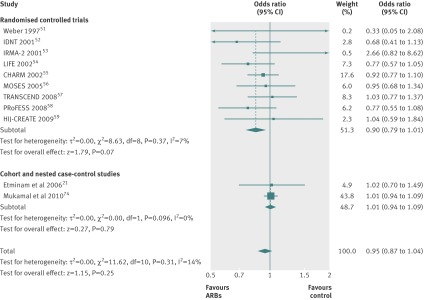
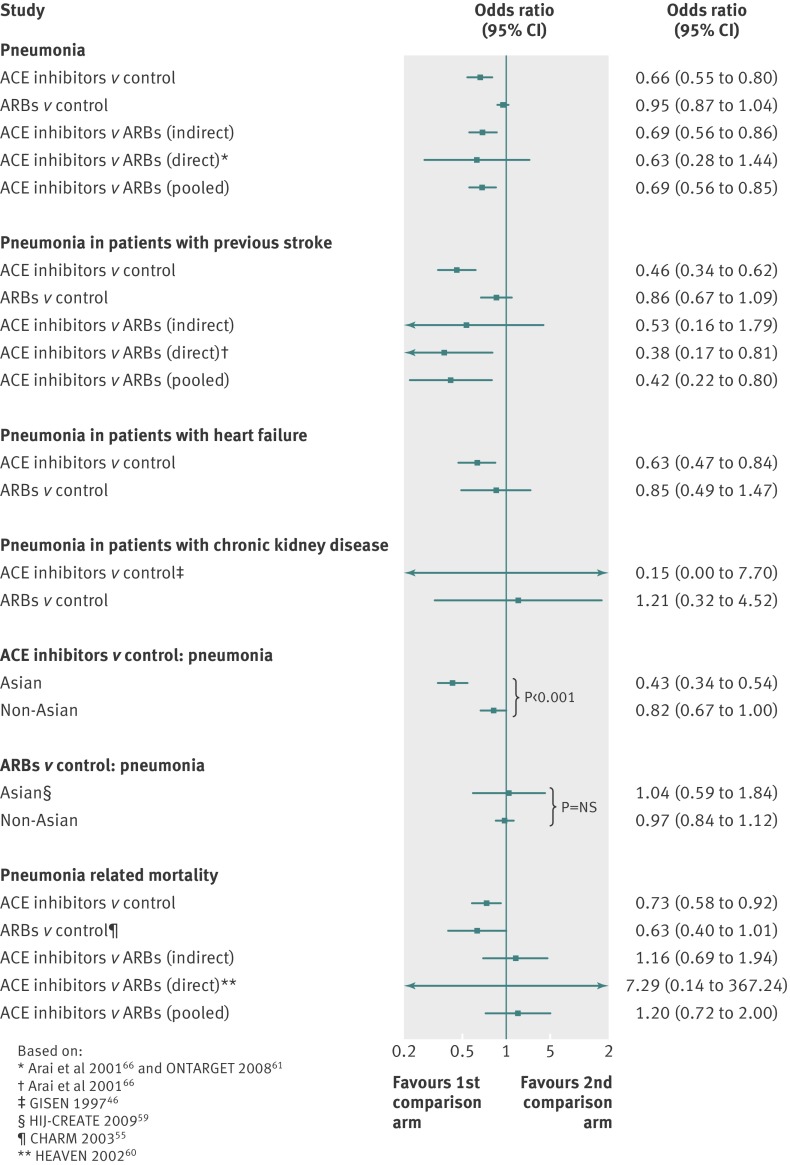
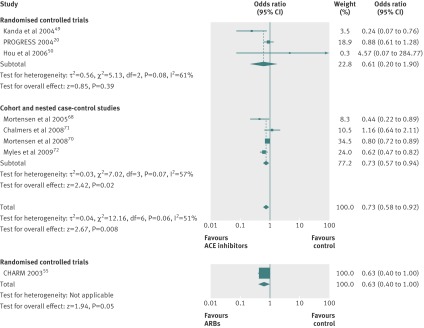
Results: 37 eligible studies were included. ACE inhibitors were associated with a significantly reduced risk of pneumonia compared with control treatment (19 studies: odds ratio 0.66, 95% confidence interval 0.55 to 0.80; I(2) = 79%) and ARBs (combined direct and indirect odds ratio estimate 0.69, 0.56 to 0.85). In patients with stroke, the risk of pneumonia was also lower in those treated with ACE inhibitors compared with control treatment (odds ratio 0.46, 0.34 to 0.62) and ARBs (0.42, 0.22 to 0.80). ACE inhibitors were associated with a significantly reduced risk of pneumonia among Asian patients (0.43, 0.34 to 0.54) compared with non-Asian patients (0.82, 0.67 to 1.00; P<0.001). Compared with control treatments, both ACE inhibitors (seven studies: odds ratio 0.73, 0.58 to 0.92; I(2)=51%) and ARBs (one randomised controlled trial: 0.63, 0.40 to 1.00) were associated with a decrease in pneumonia related mortality, without differences between interventions.
Conclusions: The best evidence available points towards a putative protective role of ACE inhibitors but not ARBs in risk of pneumonia. Patient populations that may benefit most are those with previous stroke and Asian patients. ACE inhibitors were also associated with a decrease in pneumonia related mortality, but the data lacked strength.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Pneumonia and ACE inhibitors--and cough.BMJ. 2012 Jul 11;345:e4566. doi: 10.1136/bmj.e4566. BMJ. 2012. PMID: 22786936 No abstract available.
-
ACP Journal Club. Review: ACE inhibitors reduce risk for pneumonia.Ann Intern Med. 2012 Nov 20;157(10):JC5-2. doi: 10.7326/0003-4819-157-10-201211200-02002. Ann Intern Med. 2012. PMID: 23165678 No abstract available.
References
-
- Lim WS, Baudouin SV, George RC, Hill AT, Jamieson C, Le Jeune I, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax 2009;64(suppl 3):iii,1-55. - PubMed
-
- Samokhvalov AV, Irving HM, Rehm J. Alcohol consumption as a risk factor for pneumonia: a systematic review and meta-analysis. Epidemiol Infect 2010;138:1789-95. - PubMed
-
- Almirall J, Bolíbar I, Balanzó X, González CA. Risk factors for community-acquired pneumonia in adults: a population-based case-control study. Eur Respir J 1999;13:349-55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous