Modality of choice for renal replacement therapy for children with acute kidney injury: Results of a survey
- PMID: 22787314
- PMCID: PMC3391809
- DOI: 10.4103/0971-4065.97130
Modality of choice for renal replacement therapy for children with acute kidney injury: Results of a survey
Abstract
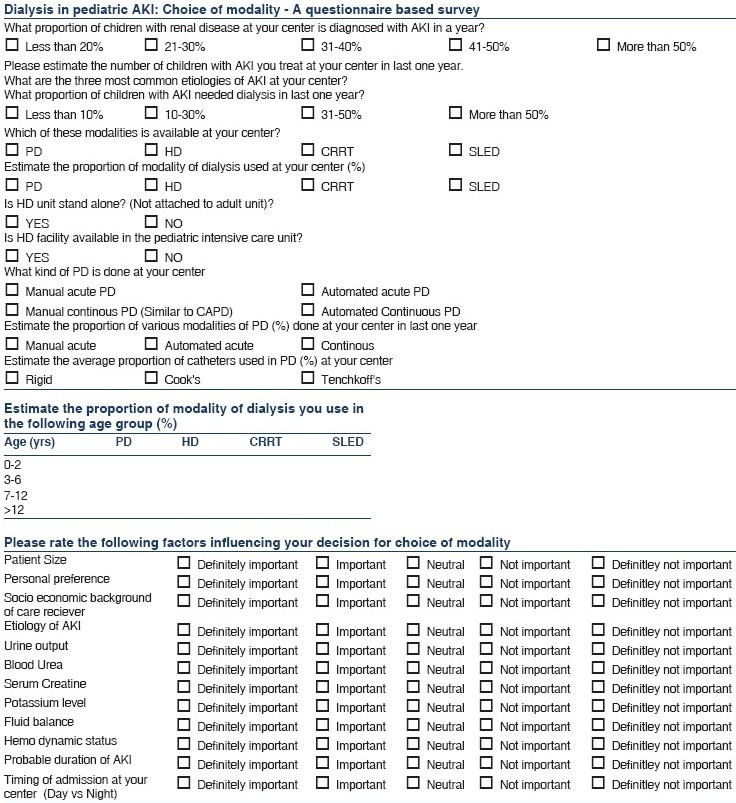
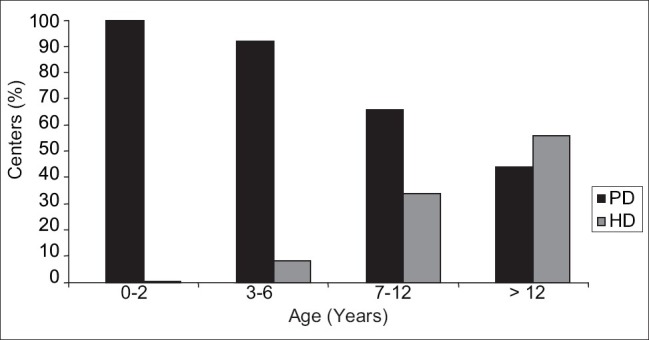
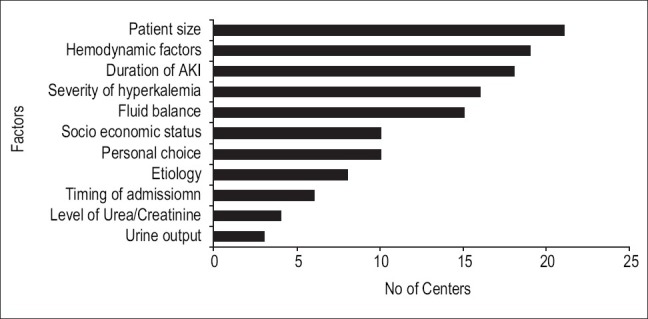
Information on current practices in India for management of renal replacement therapy (RRT) in acute kidney injury (AKI) is lacking. We mailed a questionnaire to 26 pediatric nephrology centers across India to obtain information on the current choice of dialysis modality for management of AKI in children. Acute intermittent peritoneal dialysis was available at all centers surveyed, whereas intermittent hemodialysis and continuous RRT were available in 86% and 17% centers, respectively. Peritoneal dialysis was the predominant modality (accounting for more than 80% of all dialysis) in 14 of the 22 centers, while 4 centers used hemodialysis more commonly. The most important factors influencing the modality choice were patient size, hemodynamic stability, and duration of AKI. These results provide insight into the choice of modality and factors influencing their selection in the management of pediatric AKI in our country.
Keywords: Acute kidney injury; India; renal replacement therapy; survey.
Conflict of interest statement
Figures
References
-
- Bagga A, Bakkaloglu, Devarajan P, Mehta RL, Kellum JA, Shah SV, et al. Improving outcomes from acute kidney injury: Report of an initiative. Pediatr Nephrol. 2007;22:1655–8. - PubMed
-
- Cerda J, Bagga A, Kher V, Chakravarthi RM. The contrasting characetristics of acute kidney injury in developed and developing countries. Nat Clin Pract Nephrol. 2008;4:138–53. - PubMed
-
- Maxvold NJ, Smoyer WE, Gardner JJ, Bunchman TE. Management of acute renal failure in the pediatric patient: Hemofiltration versus hemodialysis. Am J Kid Dis. 1997;5:S84–8. - PubMed
-
- Abi Antoun T, Palevsky PM. Selection of modality of renal replacement therapy. Semin Dial. 2009;22:108–13. - PubMed