Hemostatic resuscitation with plasma and platelets in trauma
- PMID: 22787340
- PMCID: PMC3391834
- DOI: 10.4103/0974-2700.96479
Hemostatic resuscitation with plasma and platelets in trauma
Abstract
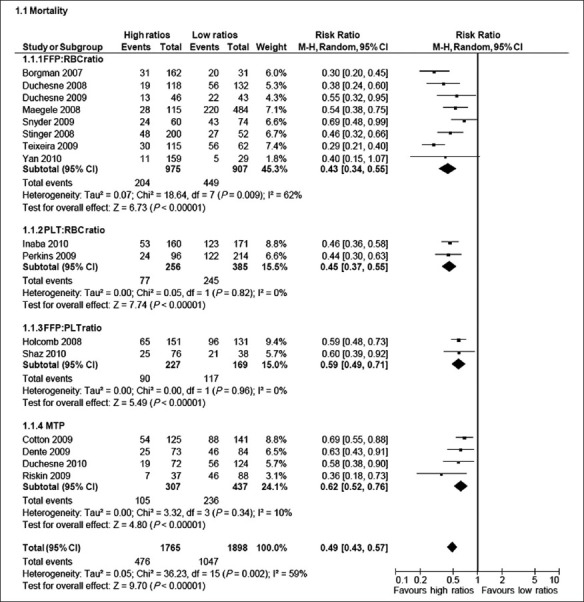
Background: Continued hemorrhage remains a major contributor of mortality in massively transfused patients and controversy regarding the optimal management exists although recently, the concept of hemostatic resuscitation, i.e., providing large amount of blood products to critically injured patients in an immediate and sustained manner as part of an early massive transfusion protocol has been introduced. The aim of the present review was to investigate the potential effect on survival of proactive administration of plasma and/or platelets (PLT) in trauma patients with massive bleeding.
Materials and methods: English databases were searched for reports of trauma patients receiving massive transfusion (10 or more red blood cell (RBC) within 24 hours or less from admission) that tested the effects of administration of plasma and/or PLT in relation to RBC concentrates on survival from January 2005 to November 2010. Comparison between highest vs lowest blood product ratios and 30-day mortality was performed.
Results: Sixteen studies encompassing 3,663 patients receiving high vs low ratios were included. This meta-analysis of the pooled results revealed a substantial statistical heterogeneity (I(2) = 58%) and that the highest ratio of plasma and/or PLT or to RBC was associated with a significantly decreased mortality (OR: 0.49; 95% confidence interval: 0.43-0.57; P<0.0001) when compared with lowest ratio.
Conclusion: Meta-analysis of 16 retrospective studies concerning massively transfused trauma patients confirms a significantly lower mortality in patients treated with the highest fresh frozen plasma (FFP) and/or PLT ratio when compared with the lowest FFP and/or PLT ratio. However, optimal ranges of FFP: RBC and PLT : RBC should be established in randomized controlled trials.
Keywords: Coagulopathy; FFP; RBC; damage control resuscitation; meta-analysis; platelet concentrate; transfusion ratios; trauma.
Conflict of interest statement
Figures
References
-
- Hardy JF, de Moerloose P, Samama M. Massive transfusion and coagulopathy: Pathophysiology and implications for clinical management. Can J Anaesth. 2004;51:293–310. - PubMed
-
- Brohi K, Cohen MJ, Ganter MT, Schultz MJ, Levi M, Mackersie RC, et al. Acute coagulopathy of trauma: Hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J Trauma. 2008;64:1211–7. - PubMed
-
- Johansson PI, Hansen MB, Sorensen H. Transfusion practice in massively bleeding patients: Time for a change? Vox Sang. 2005;89:92–6. - PubMed
-
- Hess JR, Holcomb JB, Hoyt DB. Damage control resuscitation: The need for specific blood products to treat the coagulopathy of trauma. Transfusion. 2006;46:685–6. - PubMed
-
- Deeks JJ, Higgins JP, Altman DG. Analysing data and undertaking meta-analyses. In: Higgins JP, Green S, editors. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons; 2008. pp. 243–96.
LinkOut - more resources
Full Text Sources
Medical