

One-year mortality among Danish intensive care patients with acute kidney injury: a cohort study
- PMID: 22789072
- PMCID: PMC3580703
- DOI: 10.1186/cc11420
One-year mortality among Danish intensive care patients with acute kidney injury: a cohort study
Abstract
Introduction: There are few studies on long-term mortality among intensive care unit (ICU) patients with acute kidney injury (AKI). We assessed the prevalence of AKI at ICU admission, its impact on mortality during one year of follow-up, and whether the influence of AKI varied in subgroups of ICU patients.
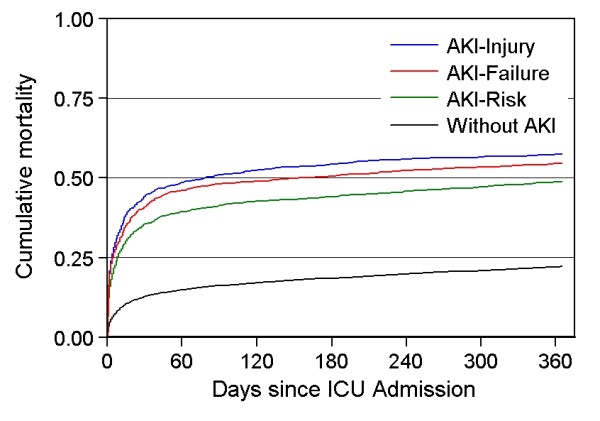
Methods: We identified all adults admitted to any ICU in Northern Denmark (approximately 1.15 million inhabitants) from 2005 through 2010 using population-based medical registries. AKI was defined at ICU admission based on the risk, injury, failure, loss of kidney function, and end-stage kidney disease (RIFLE) classification, using plasma creatinine changes. We included four severity levels: AKI-risk, AKI-injury, AKI-failure, and without AKI. We estimated cumulative mortality by the Kaplan-Meier method and hazard ratios (HRs) using a Cox model adjusted for potential confounders. We computed estimates for all ICU patients and for subgroups with different comorbidity levels, chronic kidney disease status, surgical status, primary hospital diagnosis, and treatment with mechanical ventilation or with inotropes/vasopressors.
Results: We identified 30,762 ICU patients, of which 4,793 (15.6%) had AKI at ICU admission. Thirty-day mortality was 35.5% for the AKI-risk group, 44.2% for the AKI-injury group, and 41.0% for the AKI-failure group, compared with 12.8% for patients without AKI. The corresponding adjusted HRs were 1.96 (95% confidence interval (CI) 1.80-2.13), 2.60 (95% CI 2.38 to 2.85) and 2.41 (95% CI 2.21 to 2.64), compared to patients without AKI. Among patients surviving 30 days (n = 25,539), 31- to 365 day mortality was 20.5% for the AKI-risk group, 23.8% for the AKI-injury group, and 23.2% for the AKI-failure group, compared with 10.7% for patients without AKI, corresponding to adjusted HRs of 1.33 (95% CI 1.17 to 1.51), 1.60 (95% CI 1.37 to1.87), and 1.64 (95% CI 1.42 to 1.90), respectively. The association between AKI and 30-day mortality was evident in subgroups of the ICU population, with associations persisting in most subgroups during the 31- to 365-day follow-up period, although to a lesser extent than for the 30-day period.
Conclusions: AKI at ICU admission is an important prognostic factor for mortality throughout the subsequent year.
Figures
Comment in
-
AKI patients have worse long-term outcomes, especially in the immediate post-ICU period.Crit Care. 2012 Aug 27;16(4):148. doi: 10.1186/cc11470. Crit Care. 2012. PMID: 22958588 Free PMC article.
-
Renal function after elective total hip replacement.Acta Orthop. 2016 Jun;87(3):235-8. doi: 10.3109/17453674.2016.1155130. Epub 2016 Mar 3. Acta Orthop. 2016. PMID: 26937782 Free PMC article.
References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–R212. doi: 10.1186/cc2872. - DOI - PMC - PubMed
-
- Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant. 2008;23:1203–1210. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
