

Renal function and genetic polymorphisms in pediatric heart transplant recipients
- PMID: 22789135
- PMCID: PMC3428223
- DOI: 10.1016/j.healun.2012.05.010
Renal function and genetic polymorphisms in pediatric heart transplant recipients
Abstract
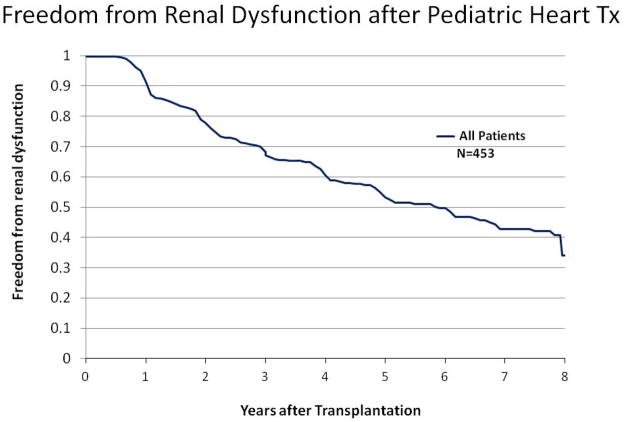
Background: Common genetic variations influence rejection, infection, drug metabolism, and side effect profiles after pediatric heart transplantation. Reports in adults suggest that genetic background may influence post-transplant renal function. In this multicenter study, we investigated the association of genetic polymorphisms (GPs) in a panel of candidate genes on renal function in 453 pediatric heart transplant recipients.
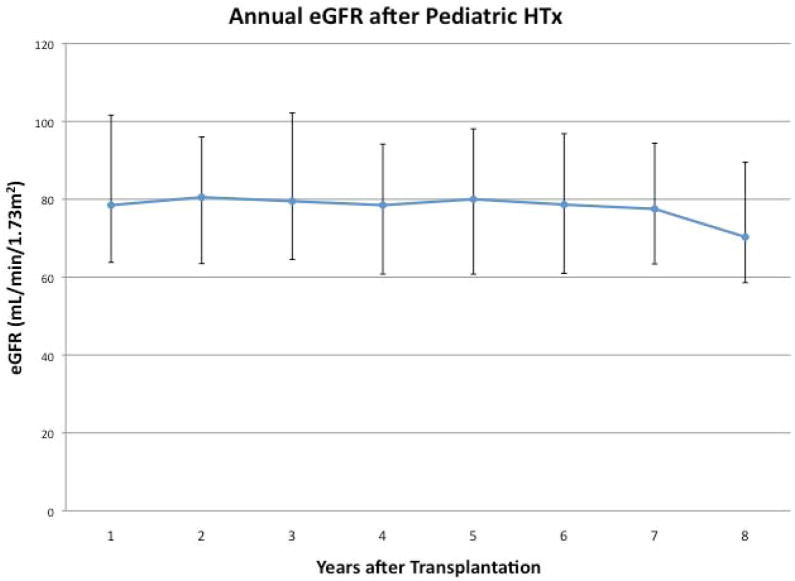
Methods: We performed genotyping for functional GPs in 19 candidate genes. Renal function was determined annually after transplantation by calculation of the estimated glomerular filtration rate (eGFR). Mixed-effects and Cox proportional hazard models were used to assess recipient characteristics and the effect of GPs on longitudinal eGFR and time to eGFR < 60 mL/min/1.73m(2).
Results: Mean age at transplantation was 6.2 ± 6.1 years. Mean follow-up was 5.1 ± 2.5 years. Older age at transplant and black race were independently associated with post-transplant renal dysfunction. Univariate analyses showed FASL (C-843T) T allele (p = 0.014) and HO-1 (A326G) G allele (p = 0.0017) were associated with decreased renal function. After adjusting for age and race, these associations were attenuated (FASL, p = 0.075; HO-1, p = 0.053). We found no associations of other GPs with post-transplant renal function, including GPs in TGFβ1, CYP3A5, ABCB1, and ACE.
Conclusions: In this multicenter, large, sample of pediatric heart transplant recipients, we found no strong associations between GPs in 19 candidate genes and post-transplant renal function. Our findings contradict reported associations of CYP3A5 and TGFβ1 with renal function and suggest that genotyping for these GPs will not facilitate individualized immunosuppression for the purpose of protecting renal function after pediatric heart transplantation.
Copyright © 2012 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Pharmacogenetics in solid organ transplantation: a transition from kinetics to dynamics.Pharmacogenomics. 2012 Nov;13(15):1679-83. doi: 10.2217/pgs.12.155. Pharmacogenomics. 2012. PMID: 23171332 No abstract available.
References
-
- Wilkinson AH, Cohen DJ. Renal failure in the recipients of nonrenal solid organ transplants. J Am Soc Nephrol. 1999 May;10(5):1136–44. - PubMed
-
- Filler G, Sharma AP. High prevalence of chronic kidney disease in pediatric solid organ transplantation. Pediatr Transplant. 2009 Feb;13(1):7–10. - PubMed
-
- Fisher NC, Nightingale PG, Gunson BK, Lipkin GW, Neuberger JM. Chronic renal failure following liver transplantation: a retrospective analysis. Transplantation. 1998;66:59–66. - PubMed
-
- Lee Ck, Christensen LL, Magee JC, Ojo AO, Harmon WE, Bridges ND. Pre-transplant Risk Factors for Chronic Renal Dysfunction After Pediatric Heart Transplantation: A 10-Year National Cohort Study. J Heart Lung Transplant. 2007;26:458–65. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
