

Neuromagnetic indicators of tinnitus and tinnitus masking in patients with and without hearing loss
- PMID: 22791191
- PMCID: PMC3441951
- DOI: 10.1007/s10162-012-0340-5
Neuromagnetic indicators of tinnitus and tinnitus masking in patients with and without hearing loss
Abstract
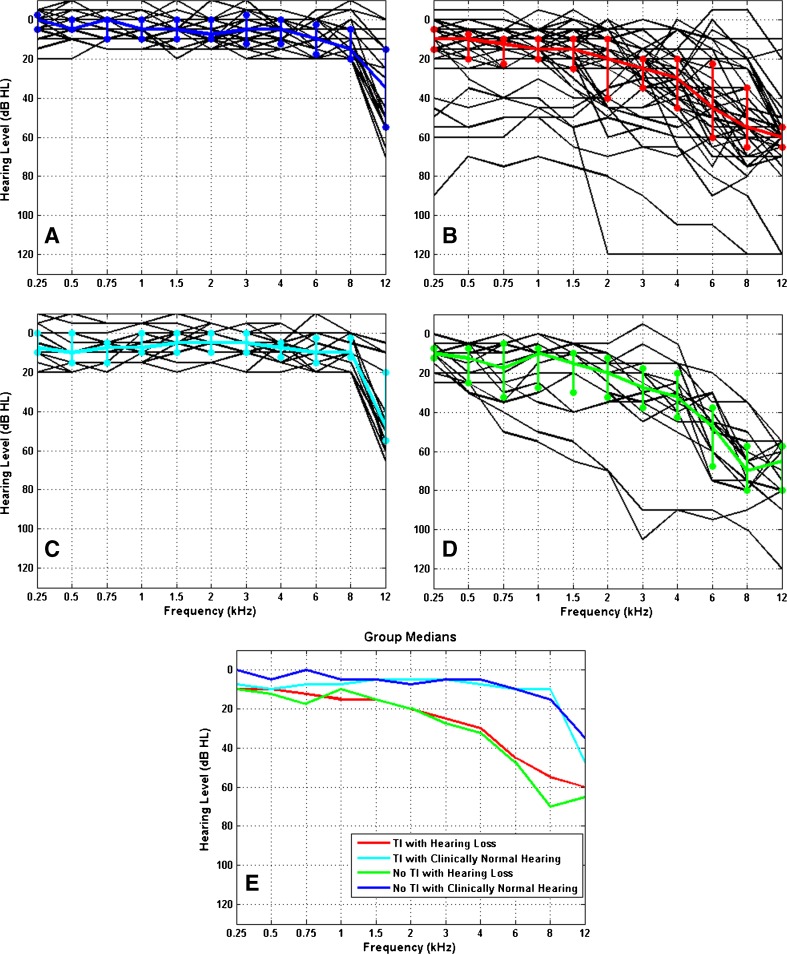
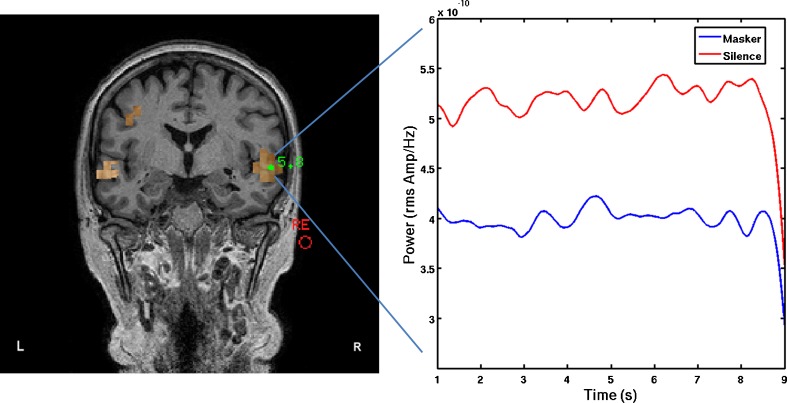
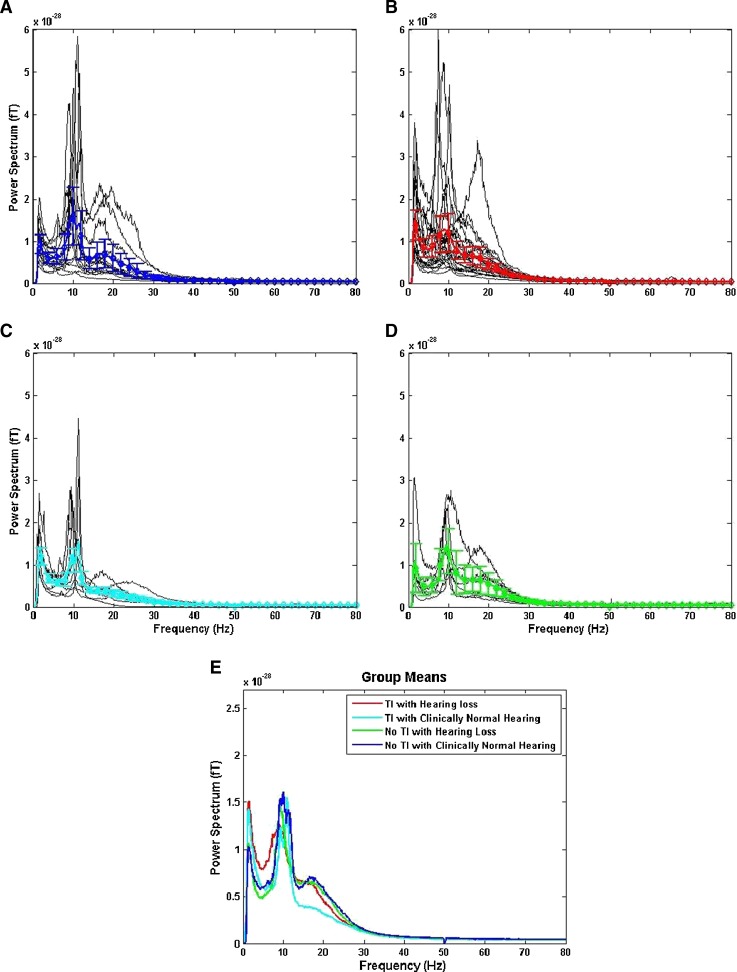
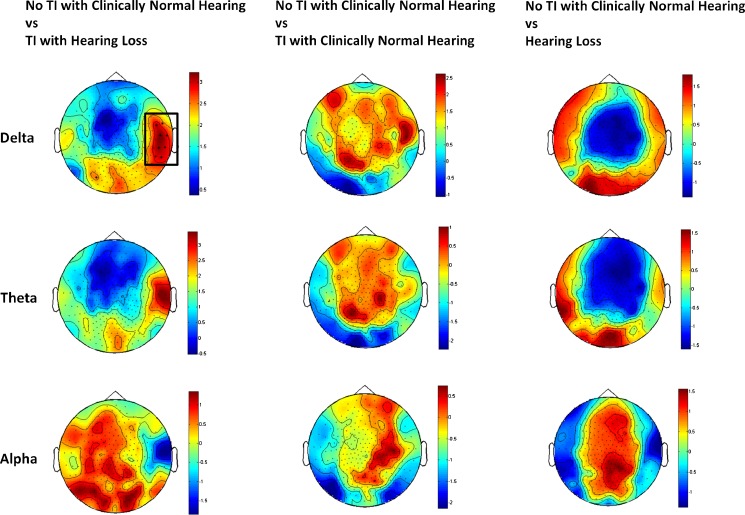
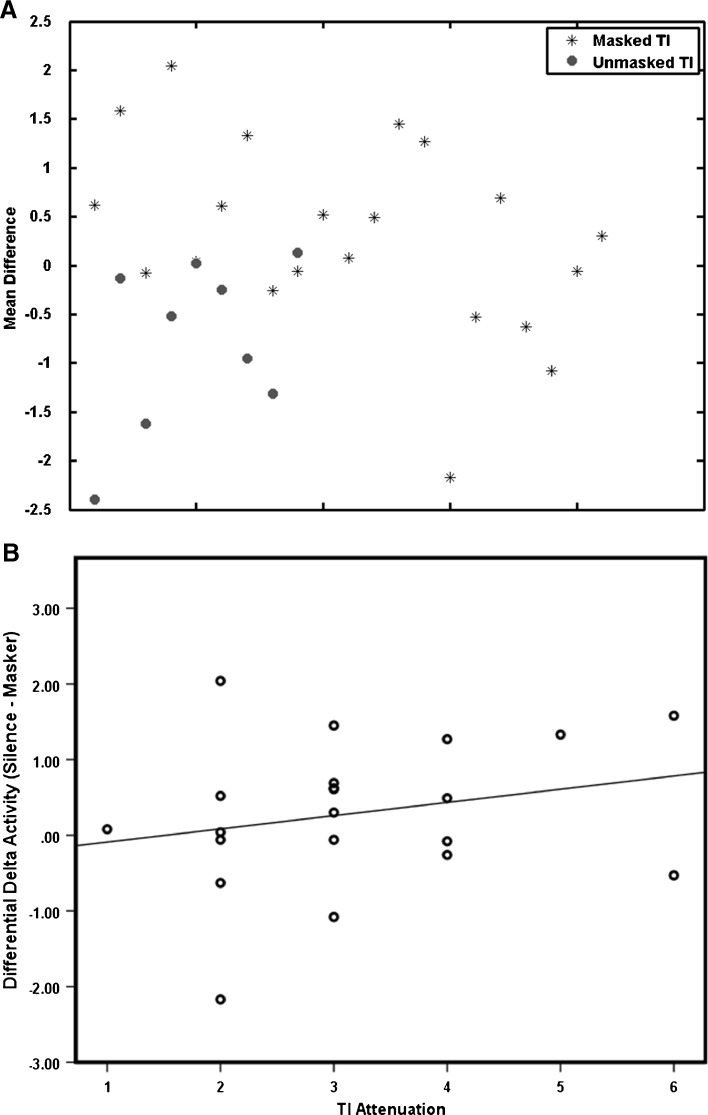
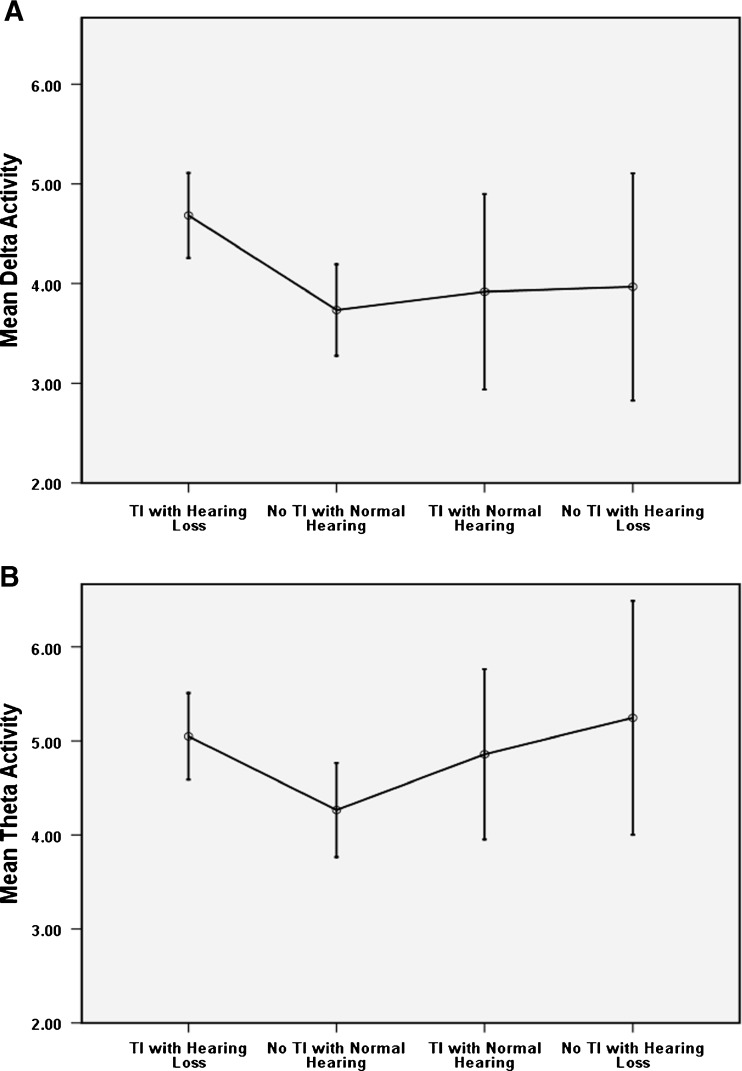
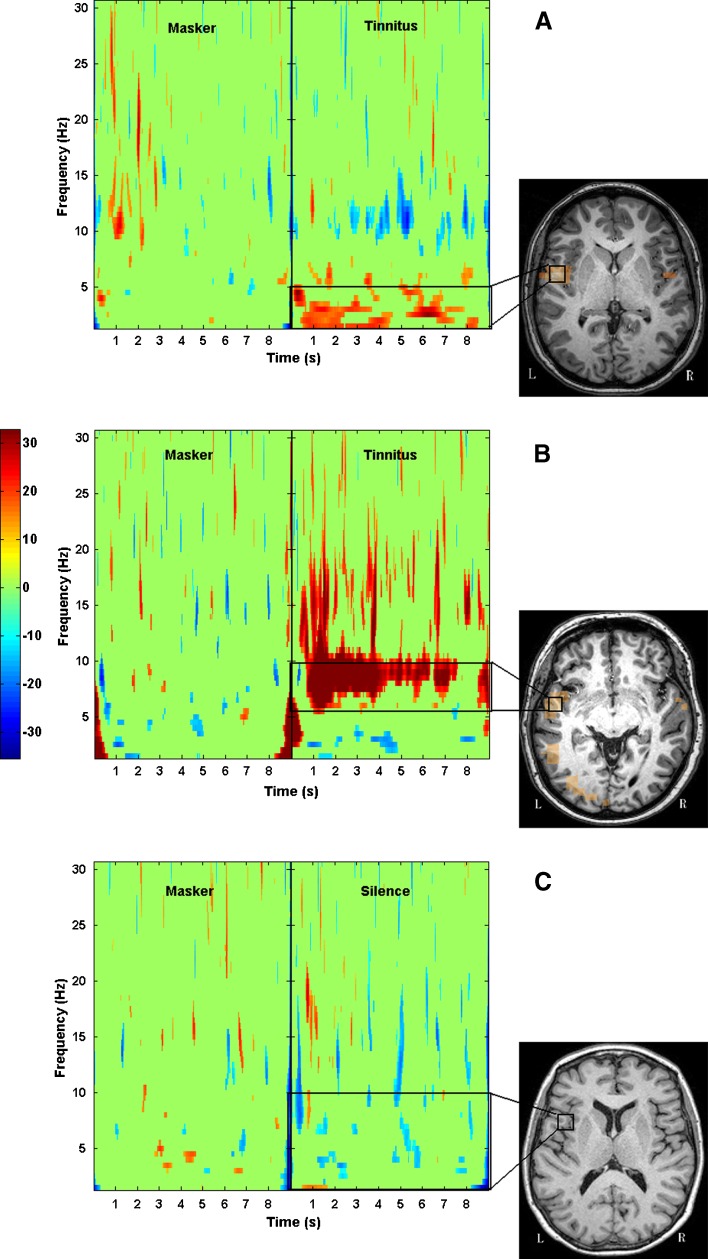
Tinnitus is an auditory phenomenon characterised by the perception of a sound in the absence of an external auditory stimulus. Chronic subjective tinnitus is almost certainly maintained via central mechanisms, and this is consistent with observed measures of altered spontaneous brain activity. A number of putative central auditory mechanisms for tinnitus have been proposed. The influential thalamocortical dysrhythmia model suggests that tinnitus can be attributed to the disruption of coherent oscillatory activity between thalamus and cortex following hearing loss. However, the extent to which this disruption specifically contributes to tinnitus or is simply a consequence of the hearing loss is unclear because the necessary matched controls have not been tested. Here, we rigorously test several predictions made by this model in four groups of participants (tinnitus with hearing loss, tinnitus with clinically normal hearing, no tinnitus with hearing loss and no tinnitus with clinically normal hearing). Magnetoencephalography was used to measure oscillatory brain activity within different frequency bands in a 'resting' state and during presentation of a masking noise. Results revealed that low-frequency activity in the delta band (1-4 Hz) was significantly higher in the 'tinnitus with hearing loss' group compared to the 'no tinnitus with normal hearing' group. A planned comparison indicated that this effect was unlikely to be driven by the hearing loss alone, but could possibly be a consequence of tinnitus and hearing loss. A further interpretative linkage to tinnitus was given by the result that the delta activity tended to reduce when tinnitus was masked. High-frequency activity in the gamma band (25-80 Hz) was not correlated with tinnitus (or hearing loss). The findings partly support the thalamocortical dysrhythmia model and suggest that slow-wave (delta band) activity may be a more reliable correlate of tinnitus than high-frequency activity.
Figures

References
-
- Adjamian P, Barnes GR, Hillebrand A, Holliday IE, Singh KD, Furlong PL, Harrington E, Barclay CW, Route PJ. Co-registration of magnetoencephalography with magnetic resonance imaging using bite-bar-based fiducials and surface-matching. Clin Neurophysiol. 2004;115:691–698. doi: 10.1016/j.clinph.2003.10.023. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
