

Cost effectiveness of vaccination against pandemic influenza in European countries: mathematical modelling analysis
- PMID: 22791791
- PMCID: PMC3395306
- DOI: 10.1136/bmj.e4445
Cost effectiveness of vaccination against pandemic influenza in European countries: mathematical modelling analysis
Abstract
Objective: To investigate whether a single optimal vaccination strategy exists across countries to deal with a future influenza pandemic by comparing the cost effectiveness of different strategies in various pandemic scenarios for three European countries.
Design: Economic and epidemic modelling study.
Settings: General populations in Germany, the Netherlands, and the United Kingdom.
Data sources: Country specific patterns of social contact and demographic data.
Model: An age structured susceptible-exposed-infected-recovered transmission model that describes how an influenza A virus will spread in the populations of Germany, the Netherlands, and the United Kingdom.
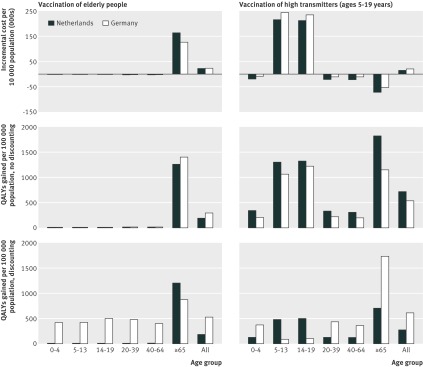
Interventions: Comparison of four vaccination strategies: no vaccination, blanket vaccination, vaccination of elderly people (≥ 65 years), and vaccination of high transmitters (5-19 years). The four strategies were evaluated for scenarios in which a vaccine became available early or at the peak of the pandemic, and in which either everyone was initially susceptible or older age groups had pre-existing immunity.
Main outcome measure: Cost per quality adjusted life years (QALYs) gained.
Results: All vaccination strategies were cost effective (incremental cost per QALY gained, comparing intervention with non-intervention). In scenarios where the vaccine became available at the peak of the pandemic and there was pre-existing immunity among elderly people the incremental cost effectiveness ratios for vaccinating high transmitters were €7325 (£5815; $10,470) per QALY gained for Germany, €10,216 per QALY gained for the Netherlands, and €7280 per QALY gained for the United Kingdom. The most cost effective strategy not only differed across the pandemic scenarios but also between countries. Specifically, when the vaccine was available early in the pandemic and there was no pre-existing immunity, in Germany it would be most cost effective to vaccinate elderly people ( €940 per QALY gained), whereas it would be most cost effective to vaccinate high transmitters in both the Netherlands (€525 per QALY gained) and the United Kingdom (€163 per QALY gained). This difference in optimal strategies was due to differences in the demographic characteristics of the countries: Germany has a significantly higher proportion of elderly people compared with the Netherlands and the United Kingdom.
Conclusions: No single vaccination strategy was most cost effective across countries. With aging populations, pre-existing immunity in particular could be of crucial importance for the cost effectiveness of options to mitigate a future influenza pandemic.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Longini IM Jr, Halloran ME, Nizam A, Yang Y. Containing pandemic influenza with antiviral agents. Am J Epidemiol 2004;159:623-33. - PubMed
-
- Mylius SD, Hagenaars TJ, Lugner AK, Wallinga J. Optimal allocation of pandemic influenza vaccine depends on age, risk and timing. Vaccine 2008;26:3742-9. - PubMed
-
- Longini IM Jr, Nizam A, Xu S, Ungchusak K, Hanshaoworakul W, Cummings DA, et al. Containing pandemic influenza at the source. Science 2005;309:1083-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical