

Patients with persistent pain after breast cancer surgery show both delayed and enhanced cortical stimulus processing
- PMID: 22792001
- PMCID: PMC3392843
- DOI: 10.2147/JPR.S30487
Patients with persistent pain after breast cancer surgery show both delayed and enhanced cortical stimulus processing
Abstract
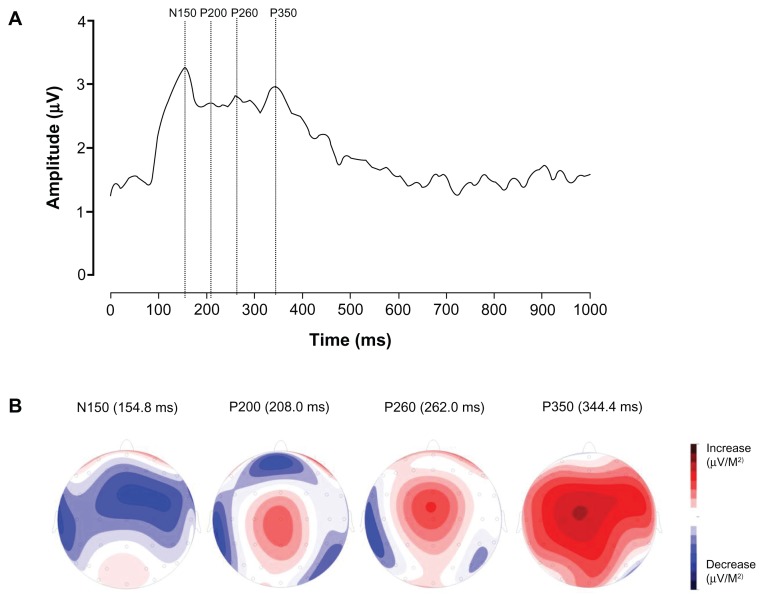
Background: Women who undergo breast cancer surgery have a high risk of developing persistent pain. We investigated brain processing of painful stimuli using electroencephalograms (EEG) to identify event-related potentials (ERPs) in patients with persistent pain after breast cancer treatment.
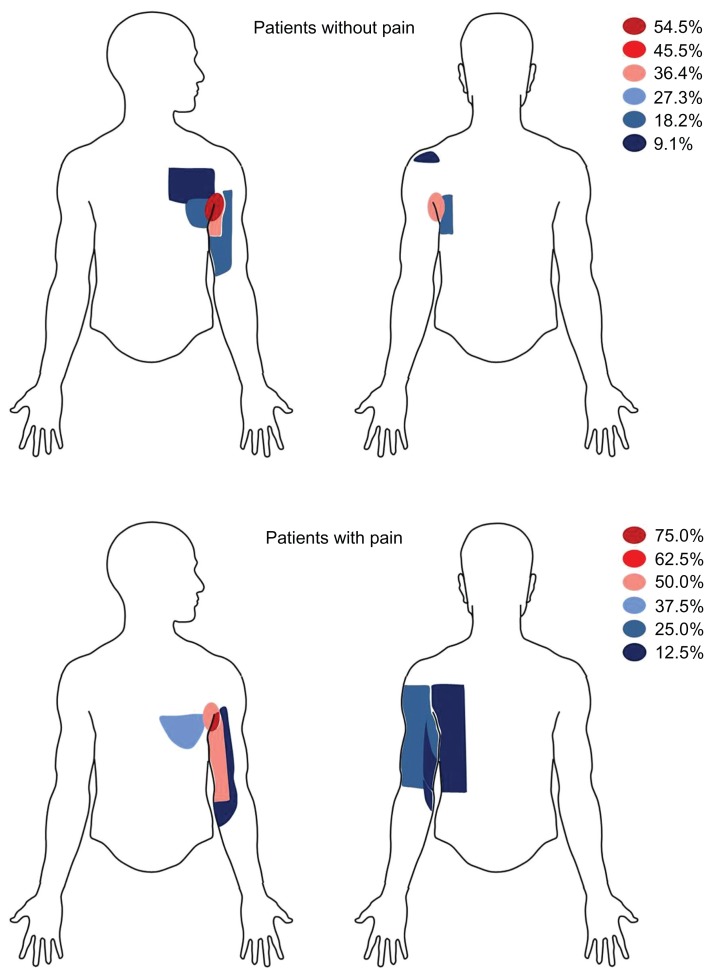
Methods: Nineteen patients (eight women with persistent pain, eleven without persistent pain), who were surgically treated more than 1 year previously for breast cancer (mastectomy, lumpectomy, and axillary lymph node dissection) and/or had chemoradiotherapy, were recruited and compared with eleven healthy female volunteers. A block of 20 painful electrical stimuli was applied to the calf, somatopically remote from the initially injured or painful area. Simultaneously an EEG was recorded, and a visual analog scale (VAS) pain rating obtained.
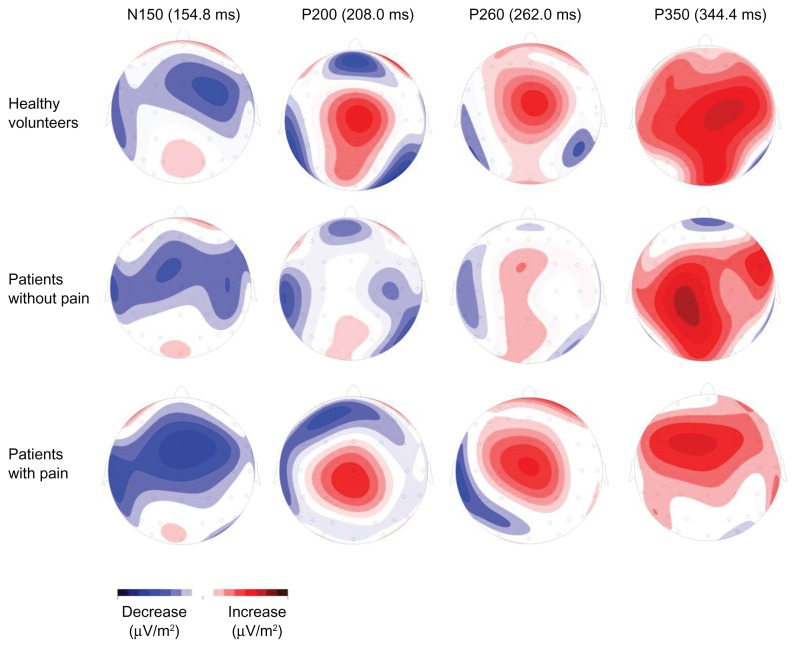
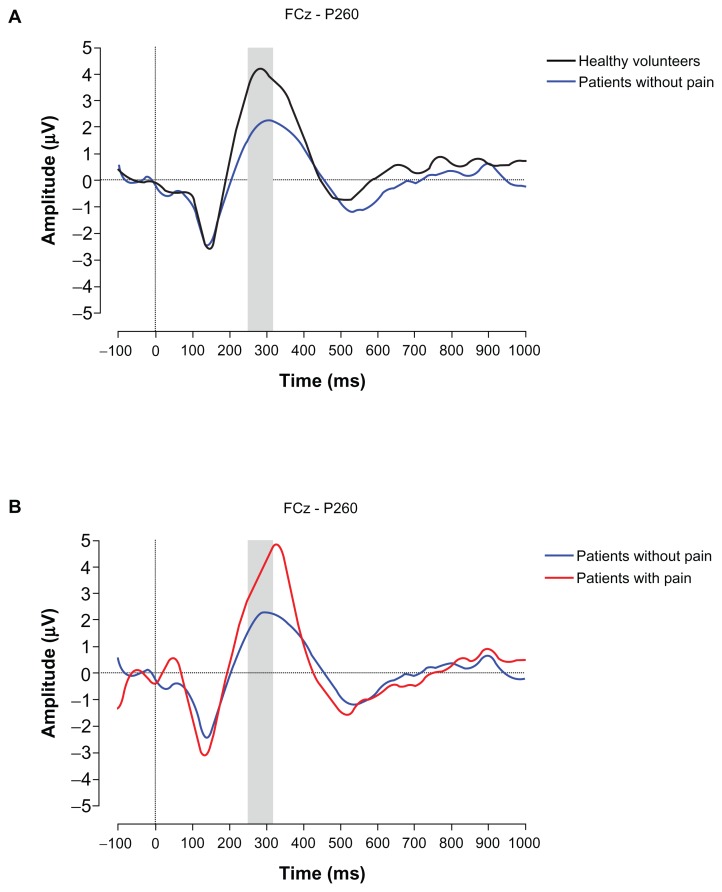
Results: In comparison with healthy volunteers, breast cancer treatment without persistent pain is associated with accelerated stimulus processing (reduced P260 latency) and shows a tendency to be less intense (lower P260 amplitude). In comparison to patients without persistent pain, persistent pain after breast cancer treatment is associated with stimulus processing that is both delayed (ie, increased latency of the ERP positivity between 250-310 ms [P260]), and enhanced (ie, enhanced P260 amplitude).
Conclusion: These results show that treatment and persistent pain have opposite effects on cortical responsiveness.
Keywords: breast cancer surgery; event-related potentials; nerve injury; pain processing; persistent pain.
Figures
Similar articles
-
Altered cortical responsiveness to pain stimuli after high frequency electrical stimulation of the skin in patients with persistent pain after inguinal hernia repair.PLoS One. 2013 Dec 23;8(12):e82701. doi: 10.1371/journal.pone.0082701. eCollection 2013. PLoS One. 2013. PMID: 24376568 Free PMC article. Clinical Trial.
-
Patients with persistent pain after breast cancer treatment show enhanced alpha activity in spontaneous EEG.Pain Med. 2013 Dec;14(12):1893-9. doi: 10.1111/pme.12216. Epub 2013 Aug 19. Pain Med. 2013. PMID: 24034712
-
Prevalence of persistent pain after breast cancer treatment by detection mode among participants in population-based screening programs.BMC Cancer. 2016 Sep 15;16(1):735. doi: 10.1186/s12885-016-2768-1. BMC Cancer. 2016. PMID: 27632982 Free PMC article.
-
Treatment of ductal carcinoma in situ: an uncertain harm-benefit balance.Prescrire Int. 2013 Dec;22(144):298-303. Prescrire Int. 2013. PMID: 24600734 Review.
-
Prevalence and intensity of persistent post-surgical pain following breast cancer surgery: a systematic review and meta-analysis of observational studies.Br J Anaesth. 2020 Sep;125(3):346-357. doi: 10.1016/j.bja.2020.04.088. Epub 2020 Jun 28. Br J Anaesth. 2020. PMID: 32611524
References
-
- Moisset X, Bouhassira D. Brain imaging of neuropathic pain. Neuroimage. 2007;37(Suppl 1):S80–S88. - PubMed
-
- Kupers R, Kehlet H. Brain imaging of clinical pain states: a critical review and strategies for future research. Lancet Neurol. 2006;5(12):1033–1044. - PubMed
-
- Steegers MA, Wolters B, Evers AW, Strobbe L, Wilder-Smith OH. The effect of axillary lymph node dissection on prevalence and intensity of chronic and phantom pain after breast cancer surgery. J Pain. 2008;9(9):813–822. - PubMed
-
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. - PubMed
LinkOut - more resources
Full Text Sources
