

Regional blockade of the shoulder: approaches and outcomes
- PMID: 22792099
- PMCID: PMC3389656
- DOI: 10.1155/2012/971963
Regional blockade of the shoulder: approaches and outcomes
Abstract
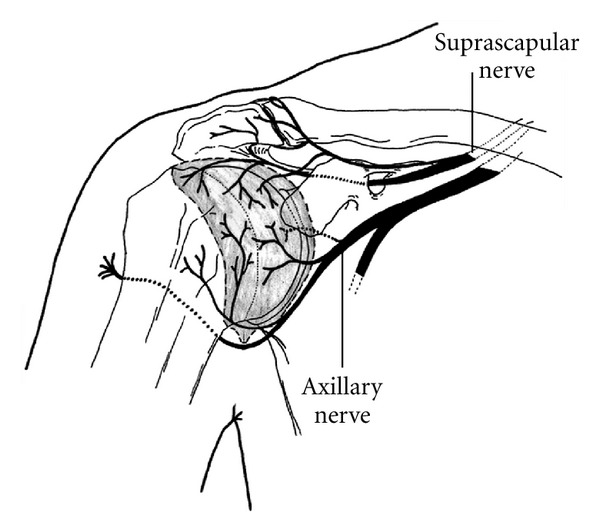
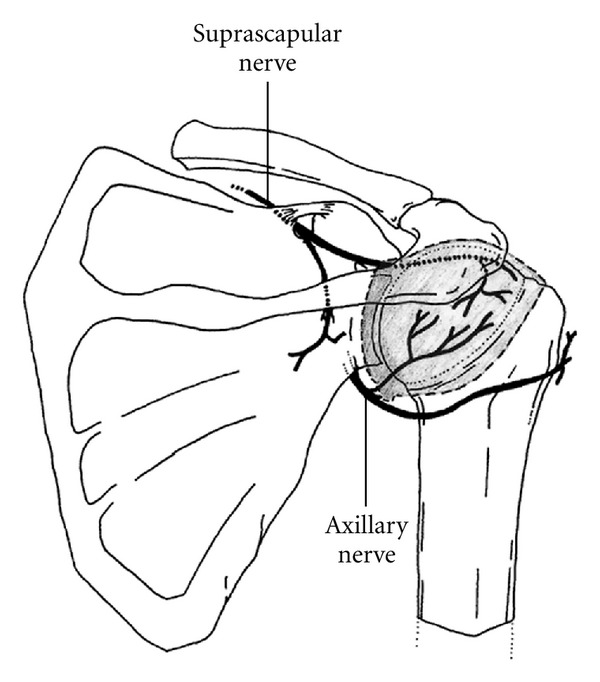
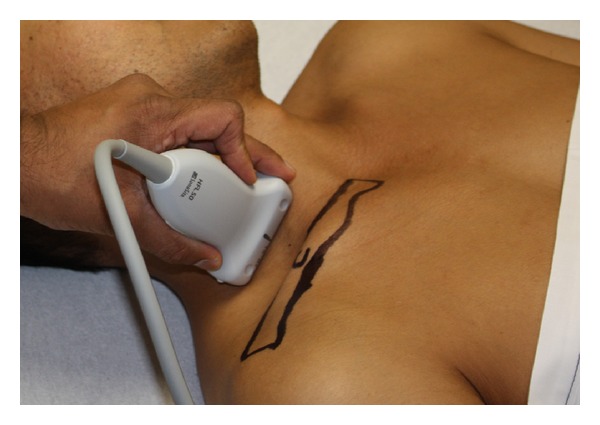
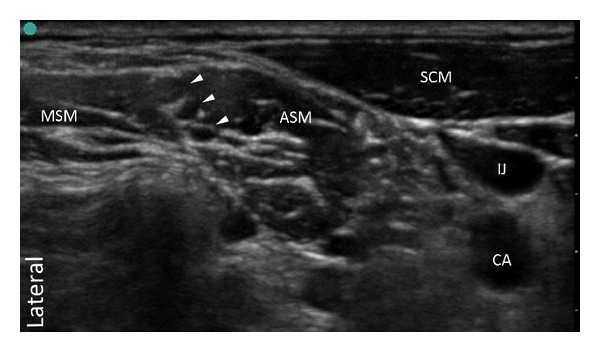
The article reviews the current literature regarding shoulder anesthesia and analgesia. Techniques and outcomes are presented that summarize our present understanding of regional anesthesia for the shoulder. Shoulder procedures producing mild to moderate pain may be managed with a single-injection interscalene block. However, studies support that moderate to severe pain, lasting for several days is best managed with a continuous interscalene block. This may cause increased extremity numbness, but will provide greater analgesia, reduce supplemental opioid consumption, improve sleep quality and patient satisfaction. In comparison to the nerve stimulation technique, ultrasound can reduce the volume of local anesthetic needed to produce an effective interscalene block. However, it has not been shown that ultrasound offers a definitive benefit in preventing major complications. The evidence indicates that the suprascapular and/or axillary nerve blocks are not as effective as an interscalene block. However in patients who are not candidates for the interscalene block, these blocks may provide a useful alternative for short-term pain relief. There is substantial evidence showing that subacromial and intra-articular injections provide little clinical benefit for postoperative analgesia. Given that these injections may be associated with irreversible chondrotoxicity, the injections are not presently recommended.
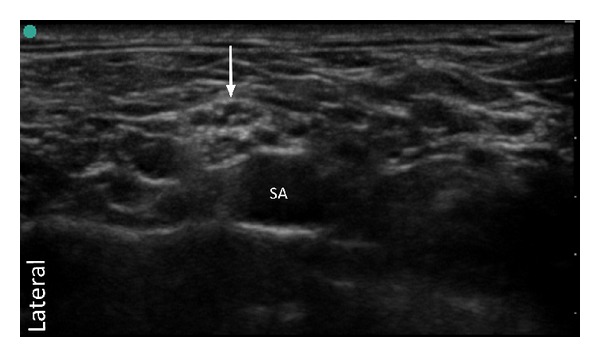
Figures
References
-
- Borgeat A, Ekatodramis G. Anaesthesia for shoulder surgery. Best Practice and Research. 2002;16(2):211–225. - PubMed
-
- Boezaart AP. Continuous interscalene block for ambulatory shoulder surgery. Best Practice and Research. 2002;16(2):295–310. - PubMed
-
- Price DJ. The shoulder block: a new alternative to interscalene brachial plexus blockade for the control of postoperative shoulder pain. Anaesthesia and Intensive Care. 2007;35(4):575–581. - PubMed
-
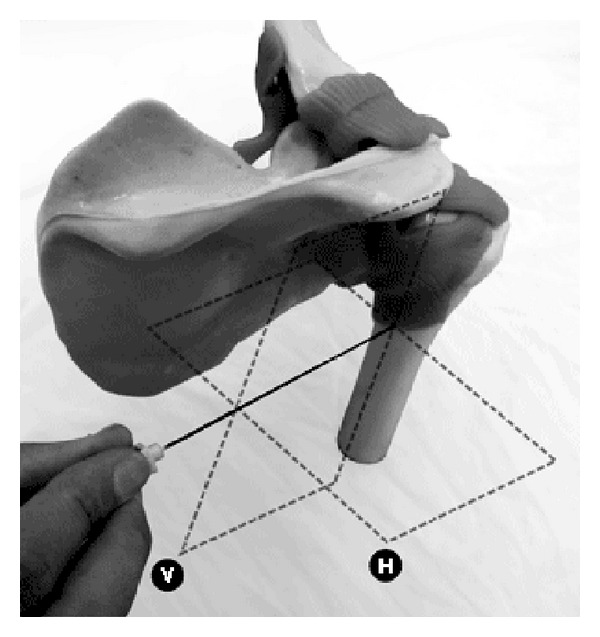
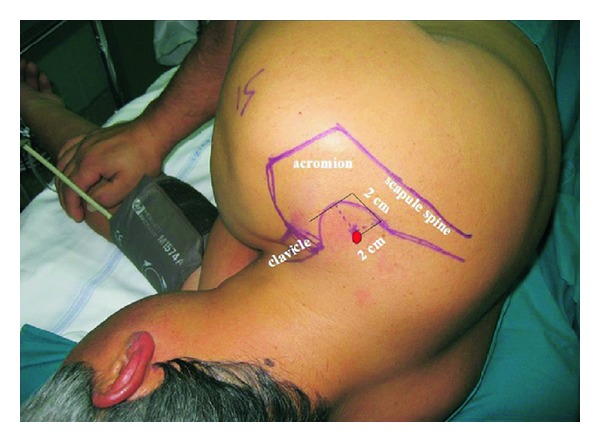
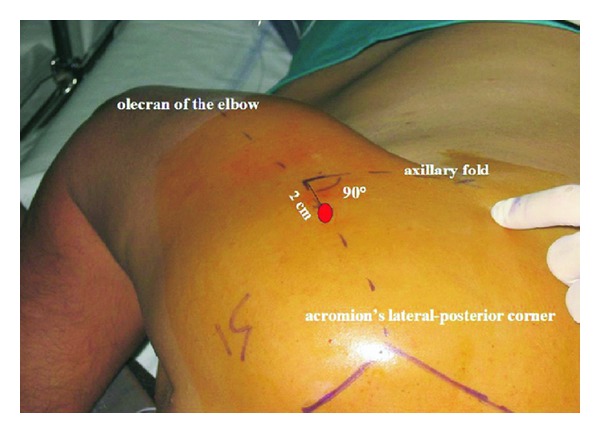
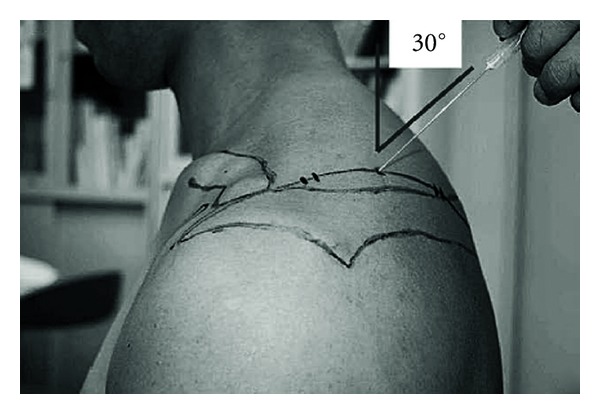
- Checcucci G, Allegra A, Bigazzi P, Gianesello L, Ceruso M, Gritti G. A new technique for regional anesthesia for arthroscopic shoulder surgery based on a suprascapular nerve block and an axillary nerve block: an evaluation of the first results. Arthroscopy. 2008;24(6):689–696. - PubMed
-
- Matsumoto D, Suenaga N, Oizumi N, Hisada Y, Minami A. A new nerve block procedure for the suprascapular nerve based on a cadaveric study. Journal of Shoulder and Elbow Surgery. 2009;18(4):607–611. - PubMed
LinkOut - more resources
Full Text Sources
Medical
