

Screening strategies for tuberculosis prevalence surveys: the value of chest radiography and symptoms
- PMID: 22792158
- PMCID: PMC3391193
- DOI: 10.1371/journal.pone.0038691
Screening strategies for tuberculosis prevalence surveys: the value of chest radiography and symptoms
Abstract
Background: We conducted a tuberculosis (TB) prevalence survey and evaluated the screening methods used in our survey, to assess if screening in TB prevalence surveys could be simplified, and to assess the accuracy of screening algorithms that may be applicable for active case finding.
Methods: All participants with a positive screen on either a symptom questionnaire, chest radiography (CXR) and/or sputum smear microscopy submitted sputum for culture. HIV status was obtained from prevalent cases. We estimated the accuracy of modified screening strategies with bacteriologically confirmed TB as the gold standard, and compared these with other survey reports. We also assessed whether sequential rather than parallel application of symptom, CXR and HIV screening would substantially reduce the number of participants requiring CXR and/or sputum culture.
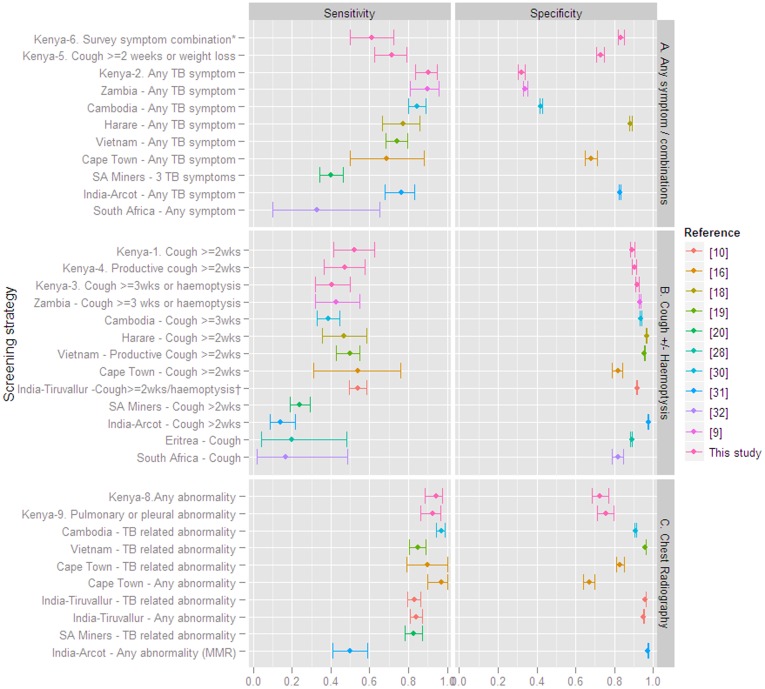
Results: Presence of any abnormality on CXR had 94% (95%CI 88-98) sensitivity (92% in HIV-infected and 100% in HIV-uninfected) and 73% (95%CI 68-77) specificity. Symptom screening combinations had significantly lower sensitivity than CXR except for 'any TB symptom' which had 90% (95%CI 84-95) sensitivity (96% in HIV-infected and 82% in HIV-uninfected) and 32% (95%CI 30-34) specificity. Smear microscopy did not yield additional suspects, thus the combined symptom/CXR screen applied in the survey had 100% (95%CI 97-100) sensitivity. Specificity was 65% (95%CI 61-68). Sequential application of first a symptom screen for 'any symptom', followed by CXR-evaluation and different suspect criteria depending on HIV status would result in the largest reduction of the need for CXR and sputum culture, approximately 36%, but would underestimate prevalence by 11%.
Conclusion: CXR screening alone had higher accuracy compared to symptom screening alone. Combined CXR and symptom screening had the highest sensitivity and remains important for suspect identification in TB prevalence surveys in settings where bacteriological sputum examination of all participants is not feasible.
Conflict of interest statement
Figures
References
-
- Glaziou P, van der Werf MJ, Onozaki I, Dye C, Borgdorff MW, et al. Tuberculosis prevalence surveys: rationale and cost. Int J Tuberc Lung Dis. 2008;12:1003–1008. - PubMed
-
- World Health Organization. TB impact measurement policy and recommendations for how to assess the epidemiological burden of TB and the impact of TB control. Geneva: World Health Organization (WHO/HTM/TB/2009.419). 2 2. 2009.
-
- van der Werf MJ, Enarson DA, Borgdorff MW. How to identify tuberculosis cases in a prevalence survey. Int J Tuberc Lung Dis. 2008;12:1255–1260. - PubMed
-
- World Health Organization. Global tuberculosis control: a short update to the 2009 report. Geneva: World Health Organization. 2009. (WHO/HTM/TB/2009.426).
-
- Pronyk PM, Joshi B, Hargreaves JR, Madonsela T, Collinson MA, et al. Active case finding: understanding the burden of tuberculosis in rural South Africa. Int J Tuberc Lung Dis. 2001;5:611–618. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
