

Central and peripheral quadriceps fatigue in congestive heart failure
- PMID: 22795722
- PMCID: PMC3776927
- DOI: 10.1016/j.ijcard.2012.06.064
Central and peripheral quadriceps fatigue in congestive heart failure
Abstract
Aims: The clinical syndrome of heart failure includes exercise limitation that is not directly linked to measures of cardiac function. Quadriceps fatigability may be an important component of this and this may arise from peripheral or central factors.
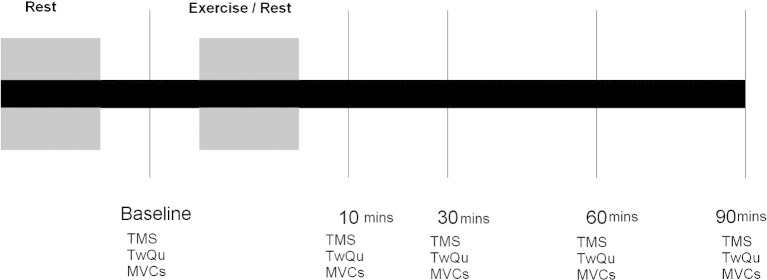
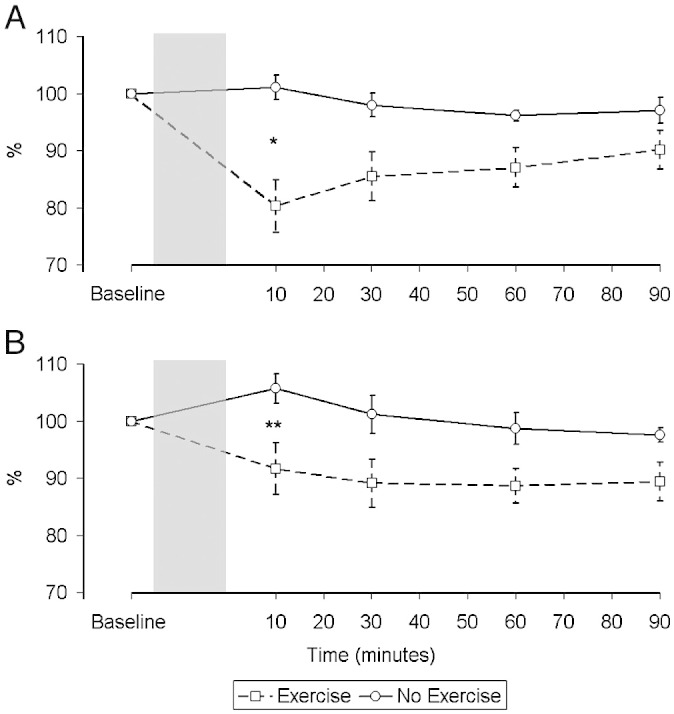
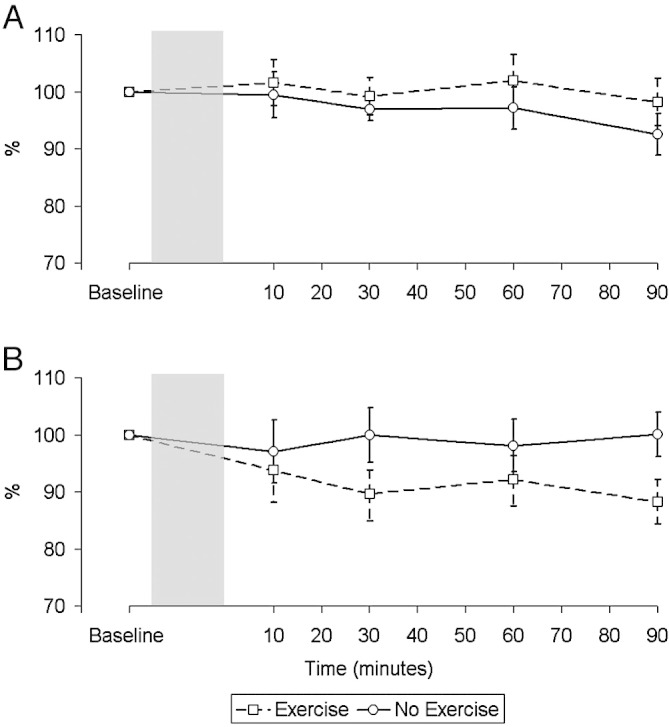
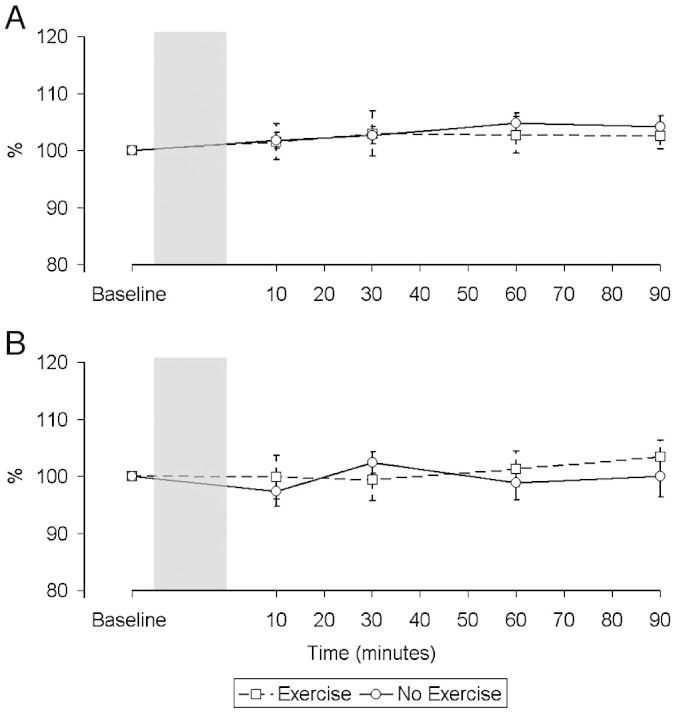
Methods and results: We studied 10 men with CHF and 10 healthy age-matched controls. Compared with a rest condition, 10 min after incremental maximal cycle exercise, twitch quadriceps force in response to supramaximal magnetic femoral nerve stimulation fell in both groups (CHF 14.1% ± 18.1%, p=0.037;
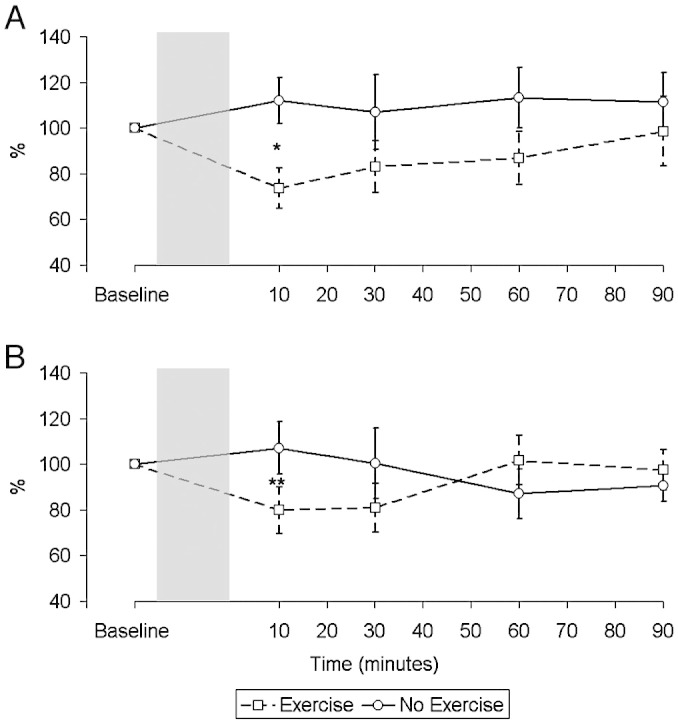
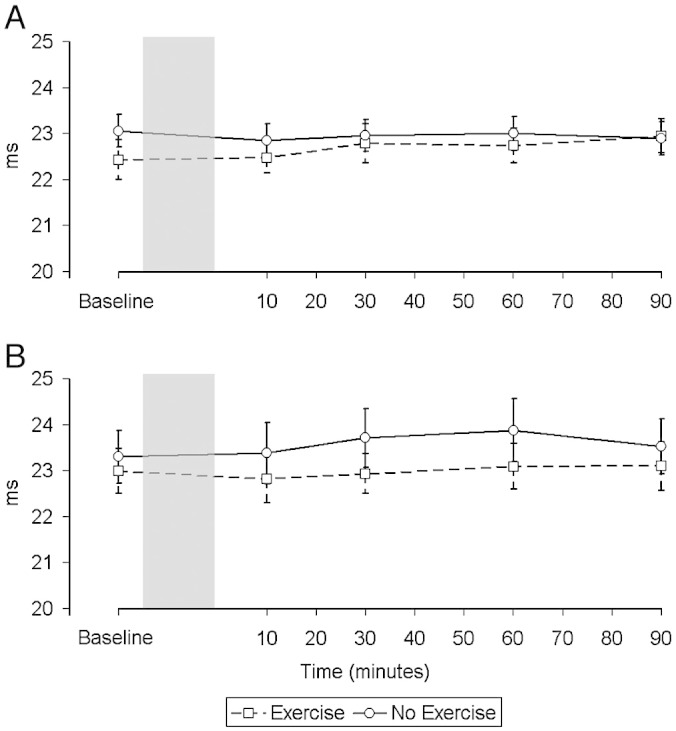
Control: 20.8 ± 11.0%, p<0.001; no significant difference between groups). There was no significant change in quadriceps maximum voluntary contraction voluntary force. The difference in the motor evoked potential (MEP) response to transcranial magnetic stimulation of the motor cortex between rest and exercise conditions at 10 min, normalised to the peripheral action potential, also fell significantly in both groups (CHF: 27.3 ± 38.7%, p=0.037;
Control: 41.1 ± 47.7%, p=0.024). However, the fall in MEP was sustained for a longer period in controls than in patients (p=0.048).
Conclusions: The quadriceps is more susceptible to fatigue, with a similar fall in TwQ occurring in CHF patients at lower levels of exercise. This is associated with no change in voluntary activation but a lesser degree of depression of quadriceps motor evoked potential.
Keywords: Brain; Exercise; Muscles; Transcranial magnetic stimulation.
Copyright © 2012 Elsevier Ireland Ltd. All rights reserved.
Figures
Similar articles
-
Central excitability does not limit postfatigue voluntary activation of quadriceps femoris.J Appl Physiol (1985). 2006 Jun;100(6):1757-64. doi: 10.1152/japplphysiol.01347.2005. Epub 2006 Jan 19. J Appl Physiol (1985). 2006. PMID: 16424071 Clinical Trial.
-
Effects of exhaustive incremental treadmill exercise on diaphragm and quadriceps motor potentials evoked by transcranial magnetic stimulation.J Appl Physiol (1985). 2004 Jan;96(1):253-9. doi: 10.1152/japplphysiol.00325.2003. Epub 2003 Sep 5. J Appl Physiol (1985). 2004. PMID: 12959961
-
Neuromuscular fatigue and exercise capacity in fibromyalgia syndrome.Arthritis Care Res (Hoboken). 2013 Mar;65(3):432-40. doi: 10.1002/acr.21845. Arthritis Care Res (Hoboken). 2013. PMID: 22965792
-
Dynamics of corticospinal changes during and after high-intensity quadriceps exercise.Exp Physiol. 2014 Aug;99(8):1053-64. doi: 10.1113/expphysiol.2014.078840. Epub 2014 Jun 6. Exp Physiol. 2014. PMID: 24907029
-
Transcranial magnetic stimulation and human muscle fatigue.Muscle Nerve. 2001 Jan;24(1):18-29. doi: 10.1002/1097-4598(200101)24:1<18::aid-mus2>3.0.co;2-d. Muscle Nerve. 2001. PMID: 11150962 Review.
Cited by
-
An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease.Am J Respir Crit Care Med. 2014 May 1;189(9):e15-62. doi: 10.1164/rccm.201402-0373ST. Am J Respir Crit Care Med. 2014. PMID: 24787074 Free PMC article. Review.
-
New device for nonvolitional evaluation of quadriceps force in ventilated patients.Muscle Nerve. 2018 May;57(5):784-791. doi: 10.1002/mus.26026. Epub 2017 Dec 11. Muscle Nerve. 2018. PMID: 29194689 Free PMC article.
-
Skeletal Muscle Fatigability in Heart Failure.Front Physiol. 2019 Feb 21;10:129. doi: 10.3389/fphys.2019.00129. eCollection 2019. Front Physiol. 2019. PMID: 30846944 Free PMC article.
-
Neuromuscular fatigue during whole body exercise.Curr Opin Physiol. 2019 Aug;10:128-136. doi: 10.1016/j.cophys.2019.05.008. Epub 2019 May 21. Curr Opin Physiol. 2019. PMID: 32818161 Free PMC article.
-
Characterization of exercise limitations by evaluating individual cardiac output patterns: a prospective cohort study in patients with chronic heart failure.BMC Cardiovasc Disord. 2015 Jun 23;15:57. doi: 10.1186/s12872-015-0057-6. BMC Cardiovasc Disord. 2015. PMID: 26100151 Free PMC article.
References
-
- Mann D.L., Bristow M.R. Mechanisms and models in heart failure. Circulation. 2005;111:2837–2849. - PubMed
-
- Carell E., Murali S., Schulman D., Estrada-Quintero T., Uretsky B. Maximal exercise tolerance in chronic congestive heart failure. Relationship to resting left ventricular function. Chest. 1994;106:1746–1752. - PubMed
-
- Lipkin D.P., Poole-Wilson P.A. Measurement of cardiac output during exercise by the thermodilution and direct Fick techniques in patients with chronic congestive heart failure. Am J Cardiol. 1985;56:321–324. - PubMed
-
- Duncan A.M., Francis D.P., Gibson D.G., Henein M.Y. Limitation of exercise tolerance in chronic heart failure: distinct effects of left Bundle–Branch block and coronary artery disease. J Am Coll Cardiol. 2004;43:1524–1531. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
