

Long-term survival and toxicity in patients treated with high-dose intensity modulated radiation therapy for localized prostate cancer
- PMID: 22795805
- PMCID: PMC5705018
- DOI: 10.1016/j.ijrobp.2012.05.023
Long-term survival and toxicity in patients treated with high-dose intensity modulated radiation therapy for localized prostate cancer
Abstract
Purpose: To report long-term survival and toxicity outcomes with the use of high-dose intensity modulated radiation therapy (IMRT) to 86.4 Gy for patients with localized prostate cancer.
Methods and materials: Between August 1997 and December 2008, 1002 patients were treated to a dose of 86.4 Gy using a 5-7 field IMRT technique. Patients were stratified by prognostic risk group based on National Comprehensive Cancer Network risk classification criteria. A total of 587 patients (59%) were treated with neoadjuvant and concurrent androgen deprivation therapy. The median follow-up for the entire cohort was 5.5 years (range, 1-14 years).
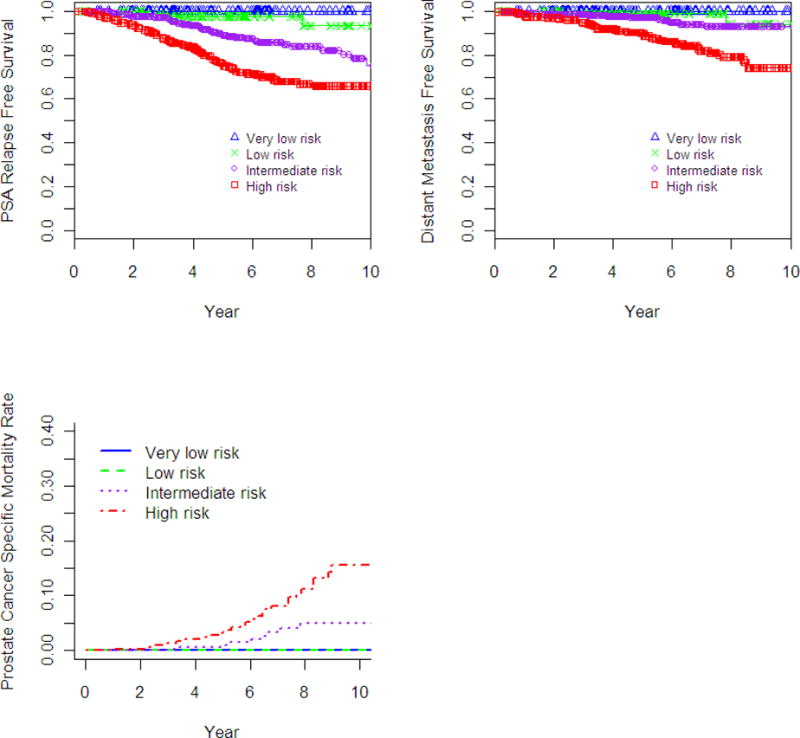
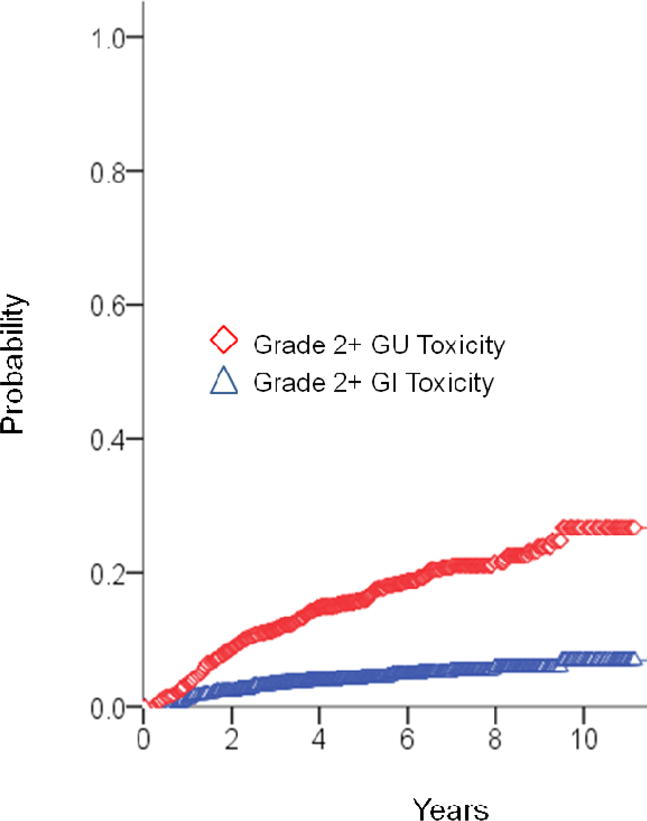
Results: For low-, intermediate-, and high-risk groups, 7-year biochemical relapse-free survival outcomes were 98.8%, 85.6%, and 67.9%, respectively (P<.001), and distant metastasis-free survival rates were 99.4%, 94.1%, and 82.0% (P<.001), respectively. On multivariate analysis, T stage (P<.001), Gleason score (P<.001), and >50% of initial biopsy positive core (P=.001) were predictive for distant mestastases. No prostate cancer-related deaths were observed in the low-risk group. The 7-year prostate cancer-specific mortality (PCSM) rates, using competing risk analysis for intermediate- and high-risk groups, were 3.3% and 8.1%, respectively (P=.008). On multivariate analysis, Gleason score (P=.004), percentage of biopsy core positivity (P=.003), and T-stage (P=.033) were predictive for PCSM. Actuarial 7-year grade 2 or higher late gastrointestinal and genitourinary toxicities were 4.4% and 21.1%, respectively. Late grade 3 gastrointestinal and genitourinary toxicity was experienced by 7 patients (0.7%) and 22 patients (2.2%), respectively. Of the 427 men with full potency at baseline, 317 men (74%) retained sexual function at time of last follow-up.
Conclusions: This study represents the largest cohort of patients treated with high-dose radiation to 86.4 Gy, using IMRT for localized prostate cancer, with the longest follow-up to date. Our findings indicate that this treatment results in excellent clinical outcomes with acceptable toxicity.
Copyright © 2013 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no financial disclosures or conflicts of interest to report.
Figures
References
-
- Rhamy RK, Wilson SK, Caldwell WL. Biopsy-proved tumor following definitive irradiation for resectable carcinoma of the prostate. J Urol. 1972;107:627–630. - PubMed
-
- Dubray BM, Beckendorf V, Guerif S, et al. Does short-term androgen depletion add to high-dose radiotherapy (80 Gy) in localized intermediate-risk prostate cancer? Intermediate analysis of GETUG 14 randomized trial (EU20503/NCT00104741) J Clin Oncol. 2011;29(suppl. 15):4521.
-
- Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:67–74. - PubMed
-
- Peeters ST, Heemsbergen WD, Koper PC, et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. 2006;24:1990–1996. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
