

Cardiac specific ATP-sensitive K+ channel (KATP) overexpression results in embryonic lethality
- PMID: 22796573
- PMCID: PMC3423334
- DOI: 10.1016/j.yjmcc.2012.07.001
Cardiac specific ATP-sensitive K+ channel (KATP) overexpression results in embryonic lethality
Abstract
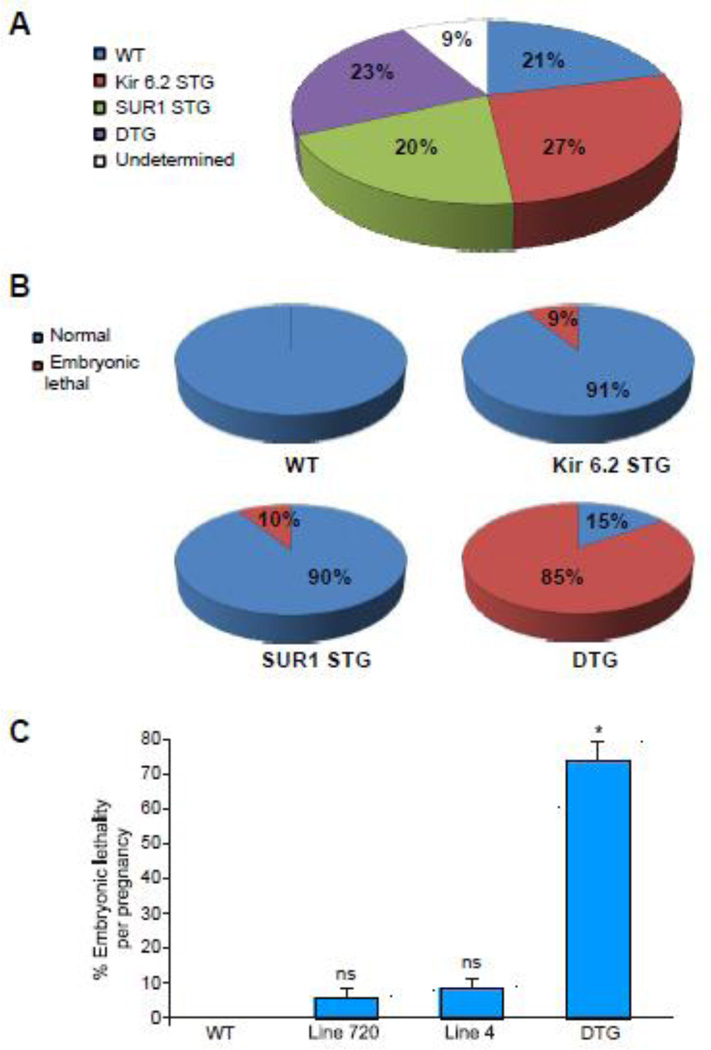
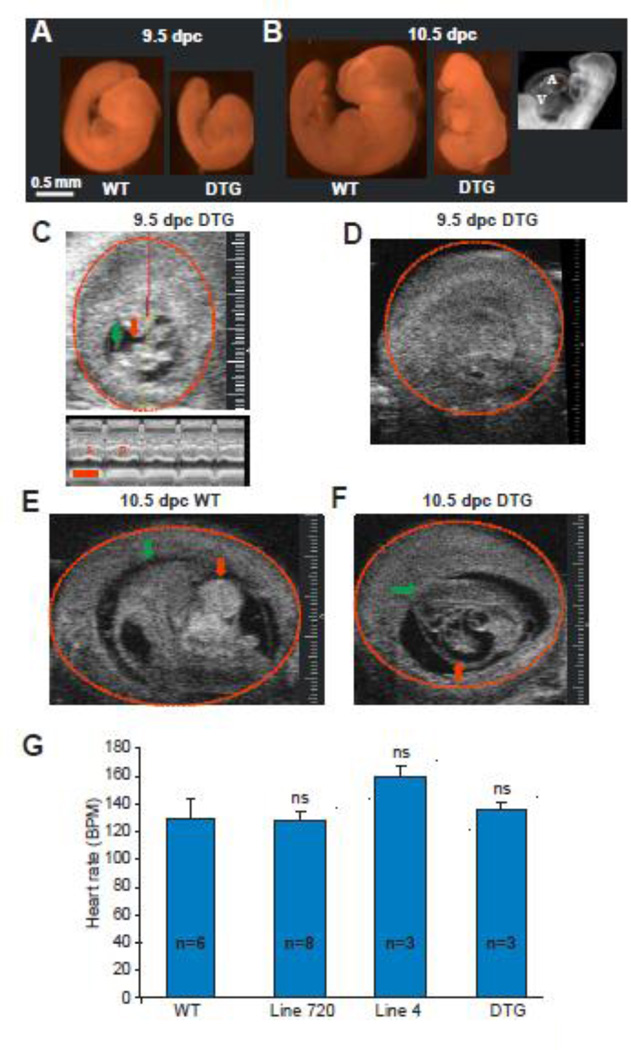
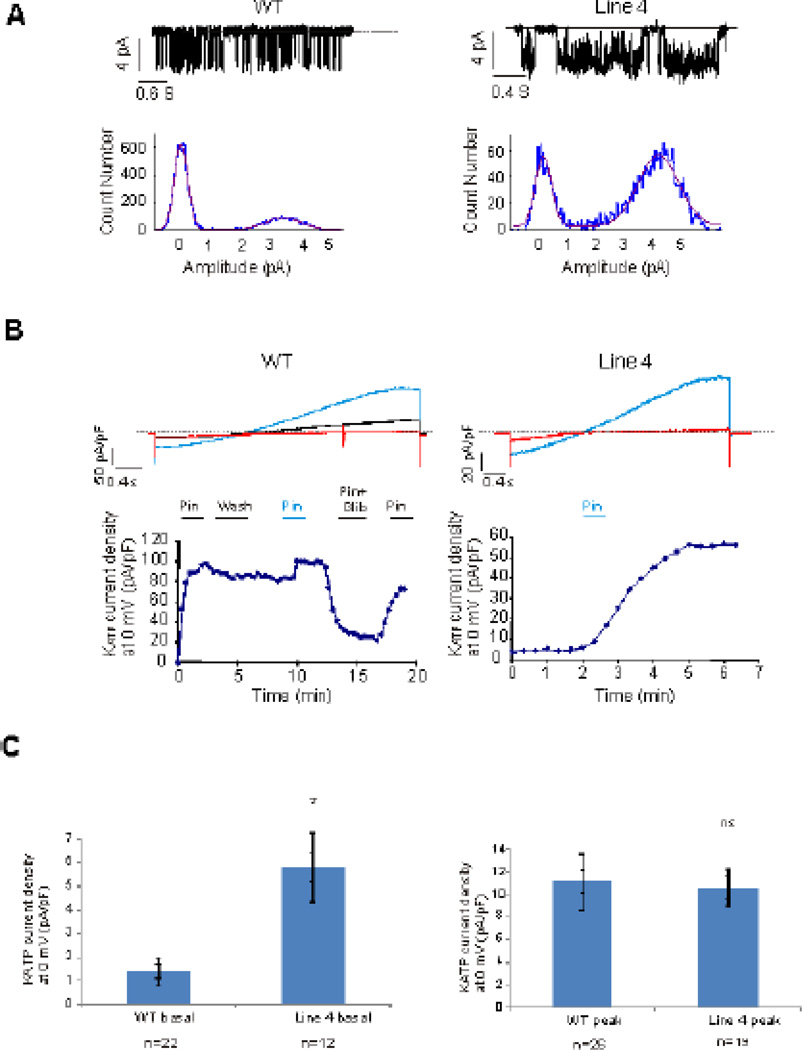
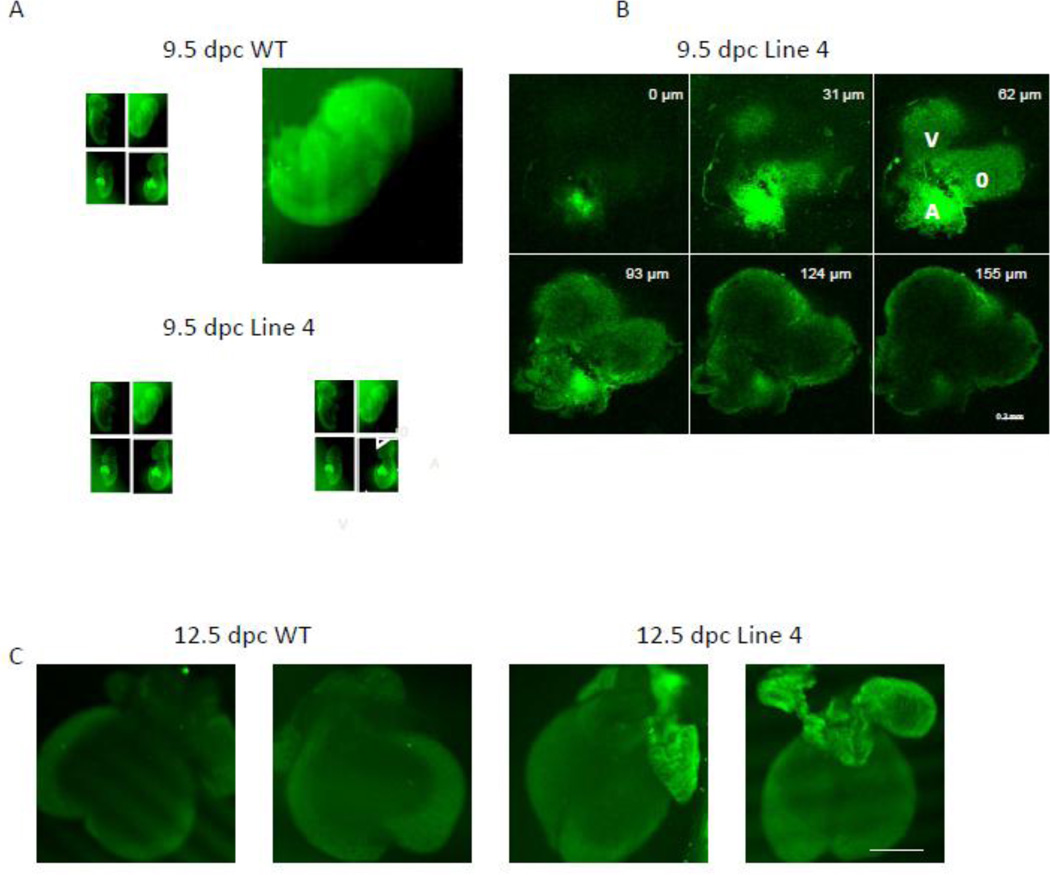
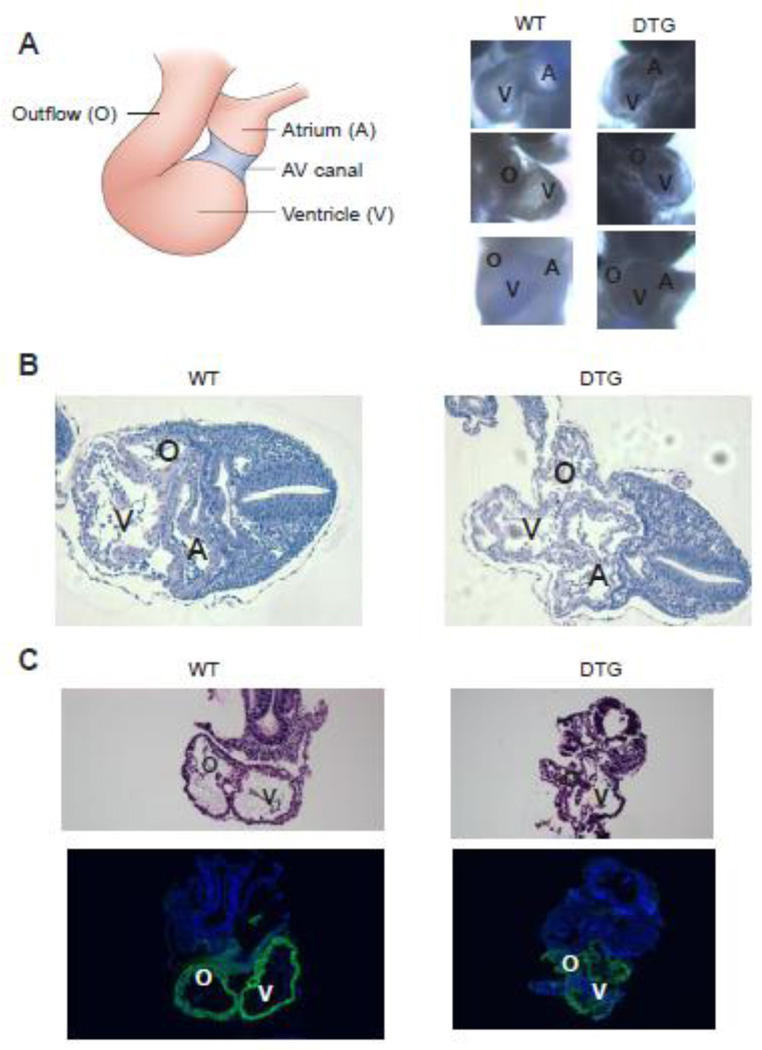
Transgenic mice overexpressing SUR1 and gain of function Kir6.2[∆N30, K185Q] K(ATP) channel subunits, under cardiac α-myosin heavy chain (αMHC) promoter control, demonstrate arrhythmia susceptibility and premature death. Pregnant mice, crossed to carry double transgenic progeny, which harbor high levels of both overexpressed subunits, exhibit the most extreme phenotype and do not deliver any double transgenic pups. To explore the fetal lethality and embryonic phenotype that result from K(ATP) overexpression, wild type (WT) and K(ATP) overexpressing embryonic cardiomyocytes were isolated, cultured and voltage-clamped using whole cell and excised patch clamp techniques. Whole mount embryonic imaging, Hematoxylin and Eosin (H&E) and α smooth muscle actin (αSMA) immunostaining were used to assess anatomy, histology and cardiac development in K(ATP) overexpressing and WT embryos. Double transgenic embryos developed in utero heart failure and 100% embryonic lethality by 11.5 days post conception (dpc). K(ATP) currents were detectable in both WT and K(ATP)-overexpressing embryonic cardiomyocytes, starting at early stages of cardiac development (9.5 dpc). In contrast to adult cardiomyocytes, WT and K(ATP)-overexpressing embryonic cardiomyocytes exhibit basal and spontaneous K(ATP) current, implying that these channels may be open and active under physiological conditions. At 9.5 dpc, live double transgenic embryos demonstrated normal looping pattern, although all cardiac structures were collapsed, probably representing failed, non-contractile chambers. In conclusion, K(ATP) channels are present and active in embryonic myocytes, and overexpression causes in utero heart failure and results in embryonic lethality. These results suggest that the K(ATP) channel may have an important physiological role during early cardiac development.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
References
-
- Zingman LV, Alekseev AE, Hodgson-Zingman DM, Terzic A. ATP-sensitive potassium channels: metabolic sensing and cardioprotection. J Appl Physiol. 2007 Nov;103(5):1888–1893. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
