

Lipid-related markers and cardiovascular disease prediction
- PMID: 22797450
- PMCID: PMC4211641
- DOI: 10.1001/jama.2012.6571
Lipid-related markers and cardiovascular disease prediction
Abstract
Context: The value of assessing various emerging lipid-related markers for prediction of first cardiovascular events is debated.
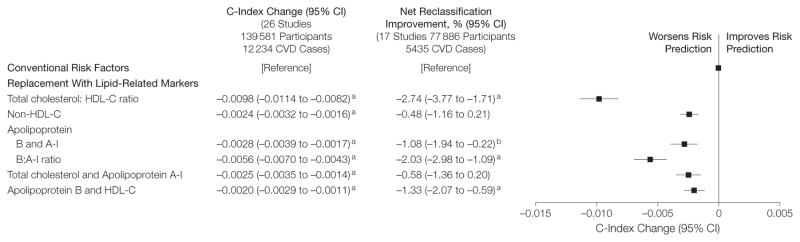
Objective: To determine whether adding information on apolipoprotein B and apolipoprotein A-I, lipoprotein(a), or lipoprotein-associated phospholipase A2 to total cholesterol and high-density lipoprotein cholesterol (HDL-C) improves cardiovascular disease (CVD) risk prediction.
Design, setting, and participants: Individual records were available for 165,544 participants without baseline CVD in 37 prospective cohorts (calendar years of recruitment: 1968-2007) with up to 15,126 incident fatal or nonfatal CVD outcomes (10,132 CHD and 4994 stroke outcomes) during a median follow-up of 10.4 years (interquartile range, 7.6-14 years).
Main outcome measures: Discrimination of CVD outcomes and reclassification of participants across predicted 10-year risk categories of low (<10%), intermediate (10%-<20%), and high (≥20%) risk.
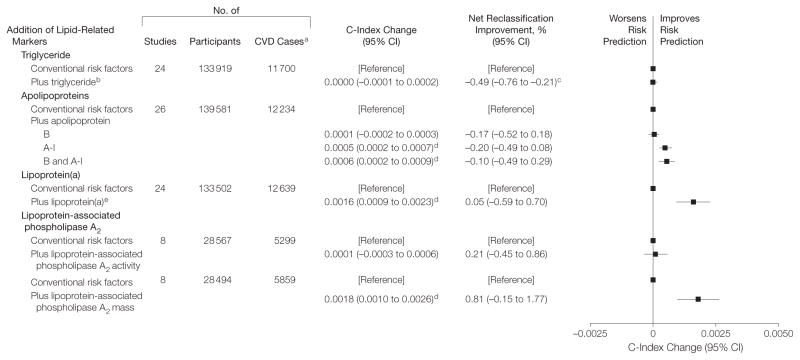
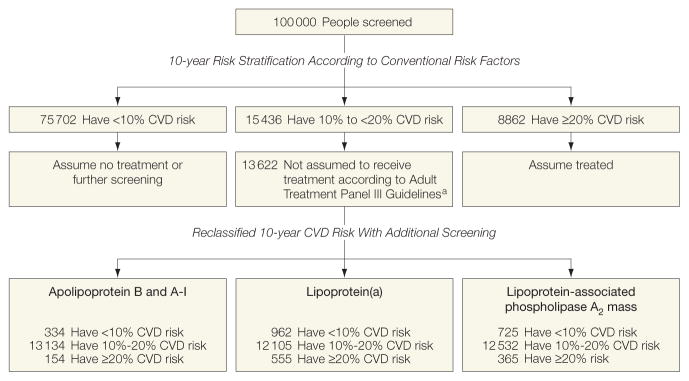
Results: The addition of information on various lipid-related markers to total cholesterol, HDL-C, and other conventional risk factors yielded improvement in the model's discrimination: C-index change, 0.0006 (95% CI, 0.0002-0.0009) for the combination of apolipoprotein B and A-I; 0.0016 (95% CI, 0.0009-0.0023) for lipoprotein(a); and 0.0018 (95% CI, 0.0010-0.0026) for lipoprotein-associated phospholipase A2 mass. Net reclassification improvements were less than 1% with the addition of each of these markers to risk scores containing conventional risk factors. We estimated that for 100,000 adults aged 40 years or older, 15,436 would be initially classified at intermediate risk using conventional risk factors alone. Additional testing with a combination of apolipoprotein B and A-I would reclassify 1.1%; lipoprotein(a), 4.1%; and lipoprotein-associated phospholipase A2 mass, 2.7% of people to a 20% or higher predicted CVD risk category and, therefore, in need of statin treatment under Adult Treatment Panel III guidelines.
Conclusion: In a study of individuals without known CVD, the addition of information on the combination of apolipoprotein B and A-I, lipoprotein(a), or lipoprotein-associated phospholipase A2 mass to risk scores containing total cholesterol and HDL-C led to slight improvement in CVD prediction.
Figures
Comment in
-
Use of emerging lipoprotein risk factors in assessment of cardiovascular risk.JAMA. 2012 Jun 20;307(23):2540-2. doi: 10.1001/jama.2012.6896. JAMA. 2012. PMID: 22797454 No abstract available.
-
Cardiovascular disease risk prediction factors.JAMA. 2012 Nov 21;308(19):1969; author reply 1970-1. doi: 10.1001/jama.2012.14049. JAMA. 2012. PMID: 23168814 No abstract available.
-
Cardiovascular disease risk prediction factors.JAMA. 2012 Nov 21;308(19):1969-70; author reply 1970-1. doi: 10.1001/jama.2012.14042. JAMA. 2012. PMID: 23168815 No abstract available.
References
-
- Perk J, De Backer G, Gohlke H, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012): The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) [published online May 2, 2012] Eur Heart J. doi: 10.1093/eurheartj/ehs092. - DOI - PubMed
-
- Parish S, Offer A, Clarke R, et al. Lipids and Lipoproteins and Risk of Different Vascular Events in the MRC/BHF Heart Protection Study. Circulation. 2012;125(20):2469–2478. - PubMed
-
- Arsenault BJ, Boekholdt SM, Kastelein JJP. Lipid parameters for measuring risk of cardiovascular disease. Nat Rev Cardiol. 2011;8(4):197–206. - PubMed
-
- Ridker PM, Rifai N, Cook NR, et al. Non-HDL cholesterol, apolipoproteins A-I and B100, standard lipid measures, lipid ratios, and CRP as risk factors for cardiovascular disease in women. JAMA. 2005;294 (3):326–333. - PubMed
-
- Arsenault BJ, Rana JS, Stroes ESG, et al. Beyond low-density lipoprotein cholesterol. J Am Coll Cardiol. 2009;55(1):35–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC085082/HL/NHLBI NIH HHS/United States
- G0100222/MRC_/Medical Research Council/United Kingdom
- G0501792/MRC_/Medical Research Council/United Kingdom
- MC_U137686857/MRC_/Medical Research Council/United Kingdom
- MC_U106179471/MRC_/Medical Research Council/United Kingdom
- UL1 TR000062/TR/NCATS NIH HHS/United States
- G0701863/MRC_/Medical Research Council/United Kingdom
- N01 HC085079/HL/NHLBI NIH HHS/United States
- G0701619/MRC_/Medical Research Council/United Kingdom
- MC_U105260792/MRC_/Medical Research Council/United Kingdom
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- RG/07/008/23674/BHF_/British Heart Foundation/United Kingdom
- N01 HC085080/HL/NHLBI NIH HHS/United States
- G0601284/MRC_/Medical Research Council/United Kingdom
- G19/35/MRC_/Medical Research Council/United Kingdom
- U01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- G8802774/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- RG/08/013/25942/BHF_/British Heart Foundation/United Kingdom
- G0902037/MRC_/Medical Research Council/United Kingdom
- N01 HC055222/HL/NHLBI NIH HHS/United States
- G0401527/MRC_/Medical Research Council/United Kingdom
