

Effect of silymarin (milk thistle) on liver disease in patients with chronic hepatitis C unsuccessfully treated with interferon therapy: a randomized controlled trial
- PMID: 22797645
- PMCID: PMC3683986
- DOI: 10.1001/jama.2012.8265
Effect of silymarin (milk thistle) on liver disease in patients with chronic hepatitis C unsuccessfully treated with interferon therapy: a randomized controlled trial
Abstract
Context: The botanical product silymarin, an extract of milk thistle, is commonly used by patients to treat chronic liver disease, despite scant and conflicting evidence of its efficacy.
Objective: To determine the effect of silymarin on liver disease activity in patients with chronic hepatitis C virus (HCV) infection unsuccessfully treated with interferon-based therapy.
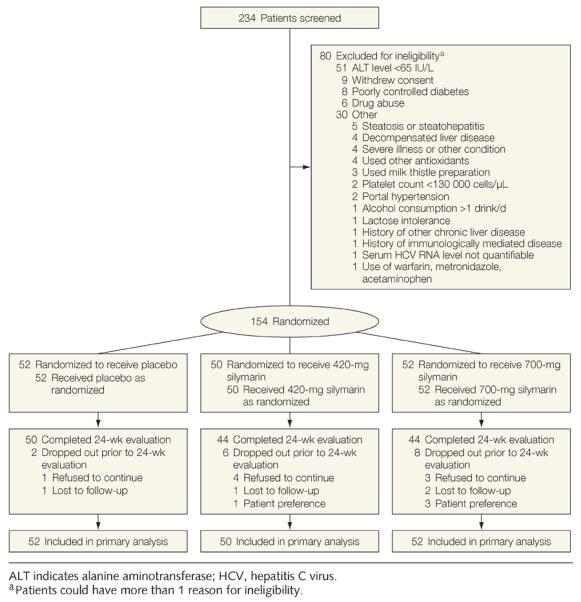
Design, setting, and participants: Multicenter, double-blind, placebo-controlled trial conducted at 4 medical centers in the United States. Participants included 154 persons with chronic HCV infection and serum alanine aminotransferase (ALT) levels of 65 U/L or greater who were previously unsuccessfully treated with interferon-based therapy. Enrollment began in May 2008 and was completed in May 2010, with the last follow-up visit completed in March 2011.
Intervention: Participants were randomly assigned to receive 420-mg silymarin, 700-mg silymarin, or matching placebo administered 3 times per day for 24 weeks.
Main outcome measures: The primary outcome measure was serum ALT level of 45 U/L or less (considered within the normal range) or less than 65 U/L, provided this was at least a 50% decline from baseline values. Secondary outcomes included changes in ALT levels, HCV RNA levels, and quality-of-life measures.
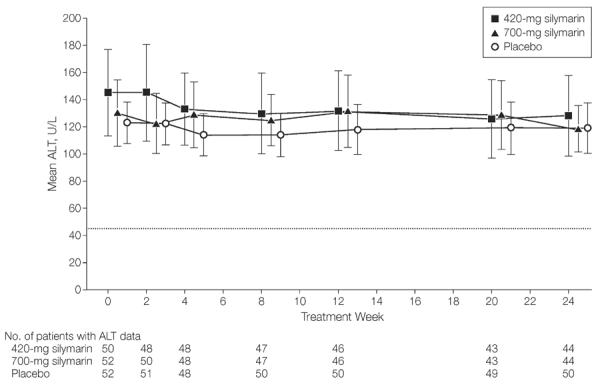
Results: After 24 weeks of treatment, only 2 participants in each treatment group (P ≥ .99) met the primary outcome measure (3.8% [95% CI, 0.5% to 13.2%] for placebo, 4.0% [95% CI, 0.5% to 13.7%] for 420-mg silymarin, and 3.8% [95% CI, 0.5% to 13.2%] for 700-mg silymarin). The mean decline in serum ALT activity at the end of treatment did not differ significantly (P = .75) across the 3 treatment groups (mean decline, -4.3 [95% CI, -17.3 to 8.7] U/L for placebo, -14.4 [95% CI, -41.6 to 12.7] U/L for 420-mg silymarin, -11.3 [95% CI, -27.9 to 5.4] U/L for 700-mg silymarin); there likewise were no significant differences in HCV RNA levels (mean change, 0.07 [95% CI, -0.05 to 0.18] log10 IU/mL for placebo, -0.03 [95% CI, -0.18 to 0.12] log10 IU/mL for 420-mg silymarin, 0.04 [95% CI, -0.08 to 0.16] log10 IU/mL for 700-mg silymarin; P = .54) or quality-of-life measures. The adverse event profile of silymarin was comparable with that of placebo.
Conclusion: Higher than customary doses of silymarin did not significantly reduce serum ALT levels more than placebo in participants with chronic HCV infection unsuccessfully treated with interferon-based therapy.
Trial registration: clinicaltrials.gov Identifier: NCT00680342.
Figures
Comment in
-
Silybin/Silymarin treatment in chronic hepatitis C.Ann Hepatol. 2012 Sep-Oct;11(5):731-3. Ann Hepatol. 2012. PMID: 22947539 No abstract available.
-
Treatment with silymarin for hepatitis C virus.JAMA. 2012 Nov 14;308(18):1856-7; author reply 1857. doi: 10.1001/jama.2012.13741. JAMA. 2012. PMID: 23149997 No abstract available.
References
-
- Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infect Dis. 2005;5(9):558–567. - PubMed
-
- Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347(13):975–982. - PubMed
-
- Jacobson IM, McHutchison JG, Dusheiko G, et al. ADVANCE Study Team Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med. 2011;364(25):2405–2416. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
