

F-18 fluorodeoxyglucose uptake and water-perfusable tissue fraction in assessment of myocardial viability
- PMID: 22797841
- PMCID: PMC3475968
- DOI: 10.1007/s12149-012-0631-2
F-18 fluorodeoxyglucose uptake and water-perfusable tissue fraction in assessment of myocardial viability
Abstract
Objectives: (15)O-water-perfusable tissue fraction (PTF) has been shown to be a potential index for assessing myocardial viability in PET, an alternative to (18)F-fluorodeoxyglucose (FDG). This study aimed to directly compare these two independent methods in assessing myocardial viability in patients with abnormal wall motion.
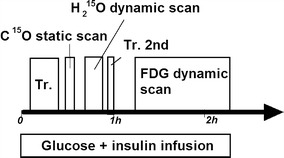
Methods: PET study was performed on 16 patients with previous myocardial infarction, before coronary artery bypass graft operation (CABG). The protocol included a (15)O-carbonmonoxide static, a (15)O-water dynamic and an (18)F-FDG dynamic scan, during the euglycemic hyperinsulinemic clamp. Echocardiography was performed at the time of PET and 5-12 months after the CABG, and the wall motion recovery was evaluated on segmental and global bases. Consistency between PTF and (18)F-FDG was evaluated visually and also in a quantitative manner. Predictive values for the wall motion recovery were also compared between the two approaches.
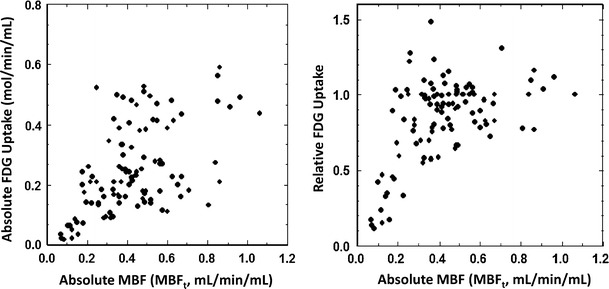
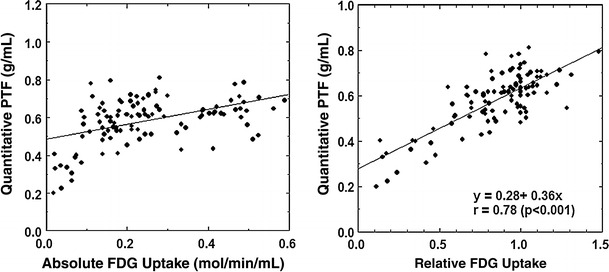
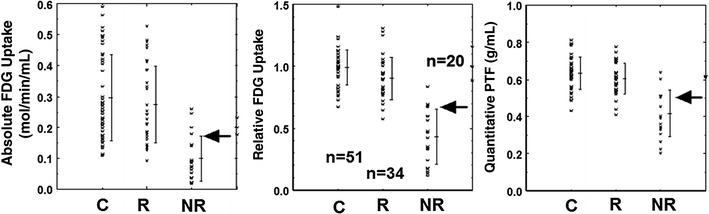
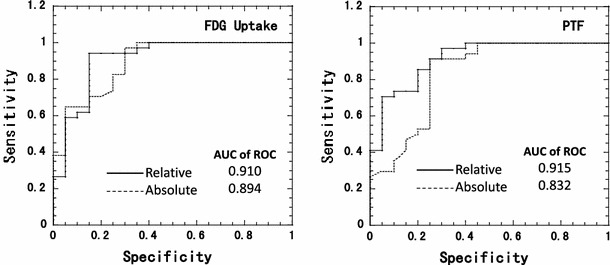
Results: The image quality of (18)F-FDG was superior to that of (15)O-water. The qualitative PTF showed significantly smaller defects than (18)F-FDG, and the quantitative PTF showed slightly greater values than (18)F-FDG in the infarcted region. The two methods were, however, consistent visually and also quantitatively. The predictive values of the wall motion recovery were almost equal between the two approaches. The absolute (18)F-FDG uptake was varied in normal segments, and predictive values for the wall motion recovery by the absolute (18)F-FDG was less (accuracy: 80 %) compared with those by the relative (18)F-FDG (accuracy: 87 %) and the quantitative PTF (accuracy: 89 %).
Conclusion: Despite the small sample size, PTF appears to give consistent results with the (18)F-FDG approach, and might be an alternative viability assessment.
Figures

References
-
- Rahimtoola SH. A perspective on the three large multicenter randomized clinical trials of coronary bypass surgery for chronic stable angina. Circulation. 1985;72(6 Pt 2):V123–V135. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
