

Medication reconciliation accuracy and patient understanding of intended medication changes on hospital discharge
- PMID: 22798200
- PMCID: PMC3475816
- DOI: 10.1007/s11606-012-2168-4
Medication reconciliation accuracy and patient understanding of intended medication changes on hospital discharge
Abstract
Background: Adverse drug events after hospital discharge are common and often serious. These events may result from provider errors or patient misunderstanding.
Objective: To determine the prevalence of medication reconciliation errors and patient misunderstanding of discharge medications.
Design: Prospective cohort study
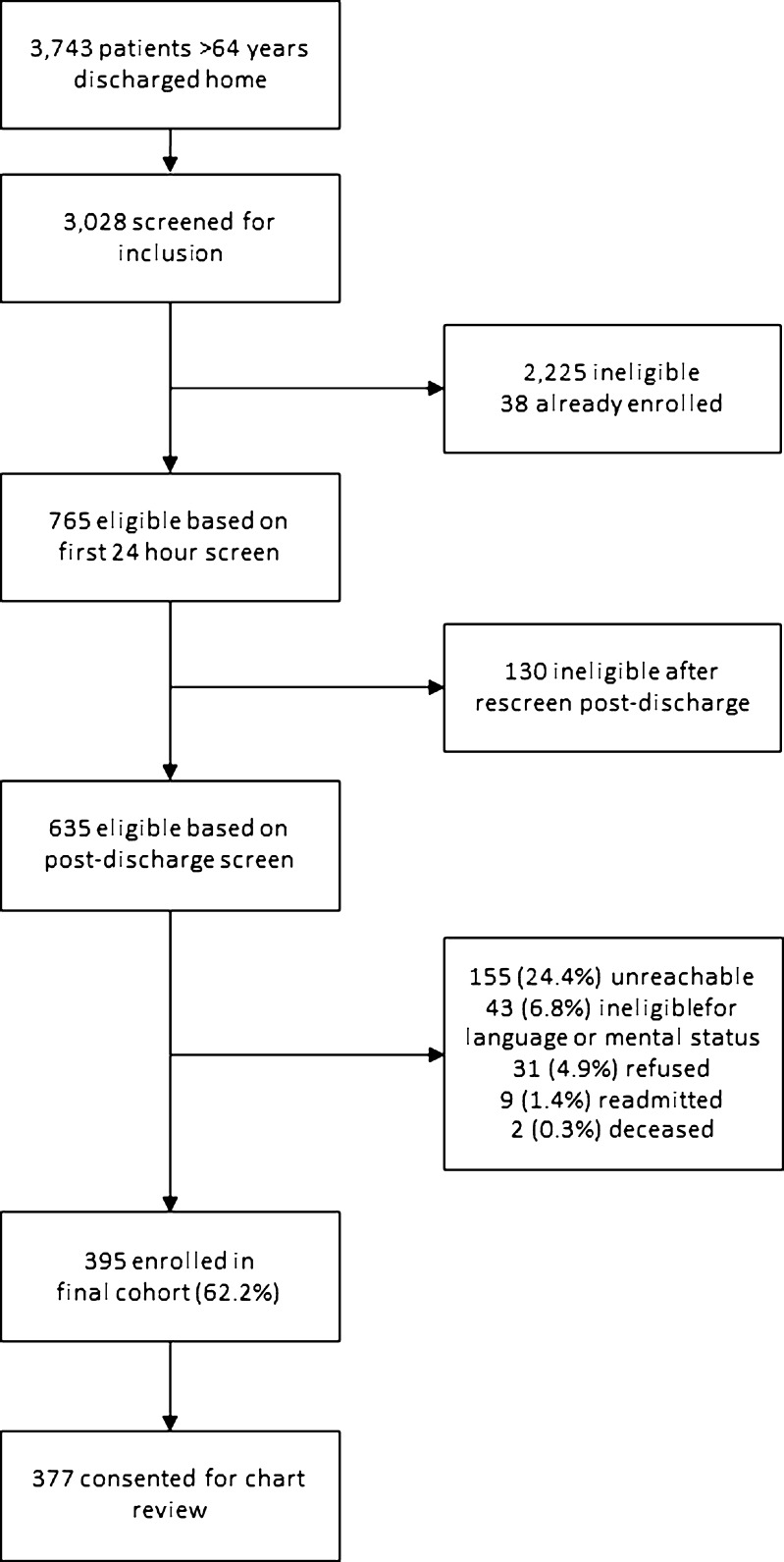
Subjects: Patients over 64 years of age admitted with heart failure, acute coronary syndrome or pneumonia and discharged to home.
Main measures: We assessed medication reconciliation accuracy by comparing admission to discharge medication lists and reviewing charts to resolve discrepancies. Medication reconciliation changes that did not appear intentional were classified as suspected provider errors. We assessed patient understanding of intended medication changes through post-discharge interviews. Understanding was scored as full, partial or absent. We tested the association of relevance of the medication to the primary diagnosis with medication accuracy and with patient understanding, accounting for patient demographics, medical team and primary diagnosis.
Key results: A total of 377 patients were enrolled in the study. A total of 565/2534 (22.3 %) of admission medications were redosed or stopped at discharge. Of these, 137 (24.2 %) were classified as suspected provider errors. Excluding suspected errors, patients had no understanding of 142/205 (69.3 %) of redosed medications, 182/223 (81.6 %) of stopped medications, and 493 (62.0 %) of new medications. Altogether, 307 patients (81.4 %) either experienced a provider error, or had no understanding of at least one intended medication change. Providers were significantly more likely to make an error on a medication unrelated to the primary diagnosis than on a medication related to the primary diagnosis (odds ratio (OR) 4.56, 95 % confidence interval (CI) 2.65, 7.85, p<0.001). Patients were also significantly more likely to misunderstand medication changes unrelated to the primary diagnosis (OR 2.45, 95 % CI 1.68, 3.55), p<0.001).
Conclusions: Medication reconciliation and patient understanding are inadequate in older patients post-discharge. Errors and misunderstandings are particularly common in medications unrelated to the primary diagnosis. Efforts to improve medication reconciliation and patient understanding should not be disease-specific, but should be focused on the whole patient.
Figures
Comment in
-
Patienten verstehen Medikationsveränderungen während der Hospitalisation nicht immer.Praxis (Bern 1994). 2013 Apr 10;102(8):487-8. doi: 10.1024/1661-8157/a001247. Praxis (Bern 1994). 2013. PMID: 23570926 German. No abstract available.
References
-
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–7. - PubMed
-
- Bell CM. Unintentional discontinuation of long-term medications for chronic diseases after hospitalization. Healthc Q. 2007;10(2):26–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
