

Respiratory infection and the impact of pulmonary immunity on lung health and disease
- PMID: 22798317
- PMCID: PMC3530220
- DOI: 10.1164/rccm.201206-1063PP
Respiratory infection and the impact of pulmonary immunity on lung health and disease
Abstract
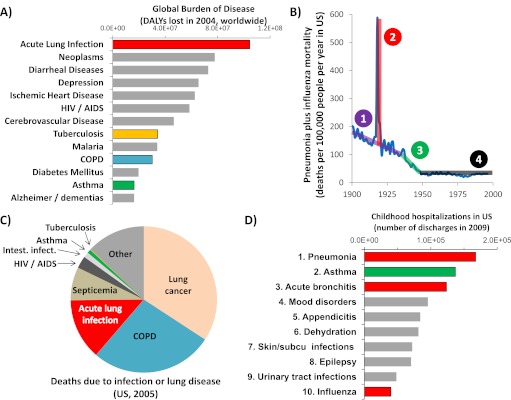
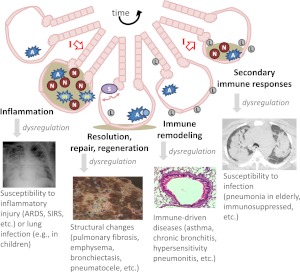
Acute lower respiratory tract infection is responsible for an inordinate disease burden. Pulmonary immunity determines the outcomes of these infections. The innate and adaptive immune responses to microbes in the lung are critical to maintaining a healthy respiratory system and preventing pulmonary disease. In addition to balancing antimicrobial defense against the risk of lung injury during the immediate infection, the shaping of pulmonary immunity by respiratory infection contributes to the pathophysiology of many and even perhaps most chronic pulmonary diseases. This Pulmonary Perspective aims to communicate two interconnected points. First, tremendous morbidity and mortality result from inadequate, misguided, or excessive pulmonary immunity. Second, our understanding of pulmonary immunity is at an exciting stage of rapid developments and discoveries, but many questions remain. Further advances in pulmonary immunity and elucidation of the cellular and molecular responses to microbes in the lung are needed to develop novel approaches to predicting, preventing, and curing respiratory disease.
Figures
References
-
- Murray CJ, Lopez AD. Evidence-based health policy–lessons from the global burden of disease study. Science 1996;274:740–743 - PubMed
-
- World Health Organization Health statistics and health information systems. 2012. [Accessed June 8, 2012]. Available from: http://www.who.int/healthinfo/global_burden_disease/estimates_regional/e...
-
- Armstrong GL, Conn LA, Pinner RW. Trends in infectious disease mortality in the United States during the 20th century. JAMA 1999;281:61–66 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
