

Impact of acute ischemic stroke treatment in patients >80 years of age: the specialized program of translational research in acute stroke (SPOTRIAS) consortium experience
- PMID: 22798327
- PMCID: PMC3429792
- DOI: 10.1161/STROKEAHA.112.660993
Impact of acute ischemic stroke treatment in patients >80 years of age: the specialized program of translational research in acute stroke (SPOTRIAS) consortium experience
Abstract
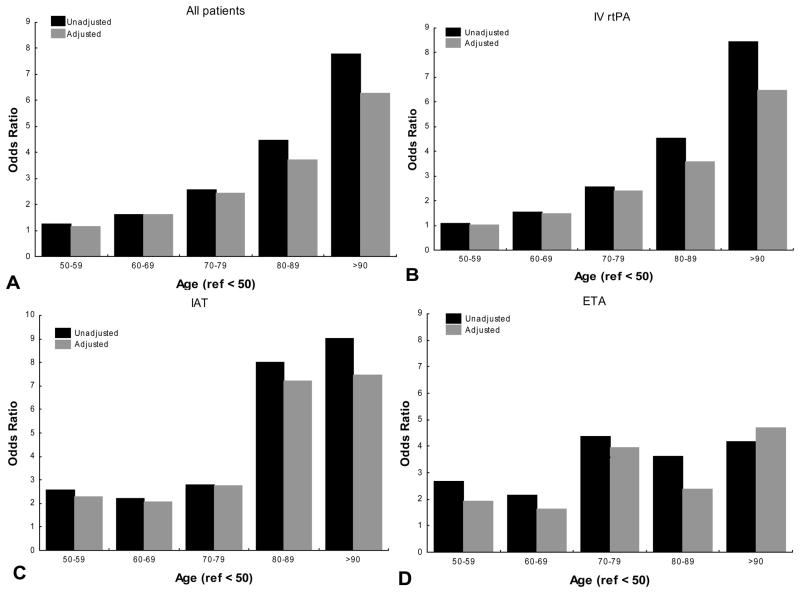
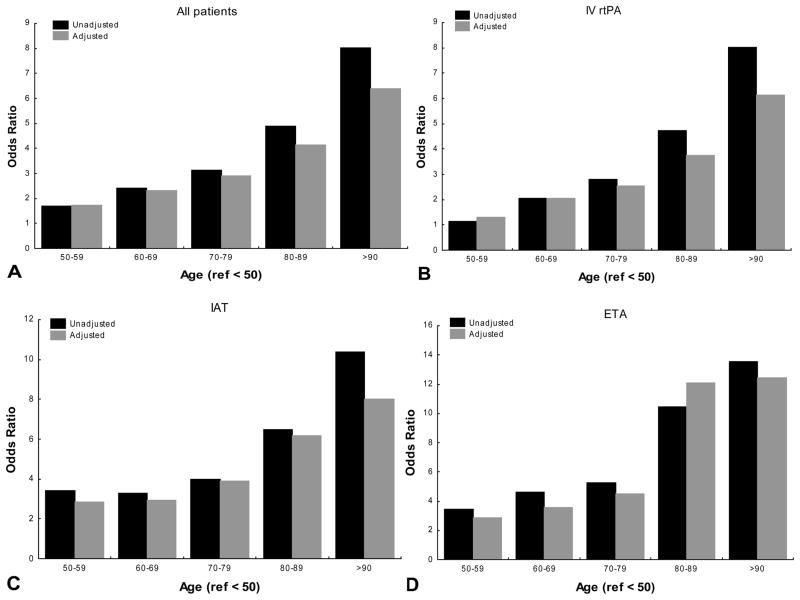
Background and purpose: Few studies have addressed outcomes among patients ≥80 years treated with acute stroke therapy. In this study, we outline in-hospital outcomes in (1) patients ≥80 years compared with their younger counterparts; and (2) those over >80 years receiving intra-arterial therapy (IAT) compared with those treated with intravenous recombinant tissue-type plasminogen activator (IV rtPA).
Methods: Stroke centers within the Specialized Program of Translational Research in Acute Stroke (SPOTRIAS) prospectively collected data on all patients treated with IV rtPA or IAT from January 1, 2005, to December 31, 2010. IAT was defined as receiving any endovascular therapy; IAT was further divided into bridging therapy when the patient received both IAT and IV rtPA and endovascular therapy alone. In-hospital mortality was compared in (1) all patients aged ≥80 years versus younger counterparts; and (2) IAT, bridging therapy, and endovascular therapy alone versus IV rtPA only among those age ≥80 years using multivariable logistic regression. An age-stratified analysis was also performed.
Results: A total of 3768 patients were included in the study; 3378 were treated with IV rtPA alone and 808 with IAT (383 with endovascular therapy alone and 425 with bridging therapy). Patients ≥80 years (n=1182) had a higher risk of in-hospital mortality compared with younger counterparts regardless of treatment modality (OR, 2.13; 95% CI, 1.60-2.84). When limited to those aged ≥80 years, IAT (OR, 0.95; 95% CI, 0.60-1.49), bridging therapy (OR, 0.82; 95% CI, 0.47-1.45), or endovascular therapy alone (OR, 1.15; 95% CI, 0.64-2.08) versus IV rtPA were not associated with increased in-hospital mortality.
Conclusions: IAT does not appear to increase the risk of in-hospital mortality among those aged >80 years compared with IV thrombolysis alone.
Figures
References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics--2008 update: A report from the american heart association statistics committee and stroke statistics subcommittee. Circulation. 2008;117:e25–146. - PubMed
-
- Lindley RI, Wardlaw JM, Sandercock PA. Thrombolysis in elderly people. Observational data insufficient to change treatment. BMJ. 2011;342:d306. author reply d312. - PubMed
-
- Fonarow GC, Smith EE, Saver JL, Reeves MJ, Bhatt DL, Grau-Sepulveda MV, et al. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: Patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation. 2011;123:750–758. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. The New England journal of medicine. 2008;359:1317–1329. - PubMed
-
- Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al. Intra-arterial prourokinase for acute ischemic stroke. The proact ii study: A randomized controlled trial. Prolyse in acute cerebral thromboembolism. Jama. 1999;282:2003–2011. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23 NS064052/NS/NINDS NIH HHS/United States
- P50 NS049060/NS/NINDS NIH HHS/United States
- K23 NS069807/NS/NINDS NIH HHS/United States
- KL2 RR024149/RR/NCRR NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- K23 NS073104/NS/NINDS NIH HHS/United States
- L30 AG031009/AG/NIA NIH HHS/United States
- KL2 TR000450/TR/NCATS NIH HHS/United States
- 1K23 NS 073104-01A1/NS/NINDS NIH HHS/United States
- N01 AG031009/AG/NIA NIH HHS/United States
- UL1 RR024148/RR/NCRR NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
