

Risk Factors for Type 2 Diabetes: Lessons Learned from Japanese Americans in Seattle
- PMID: 22798980
- PMCID: PMC3393109
- DOI: 10.1111/j.2040-1124.2012.00195.x
Risk Factors for Type 2 Diabetes: Lessons Learned from Japanese Americans in Seattle
Abstract
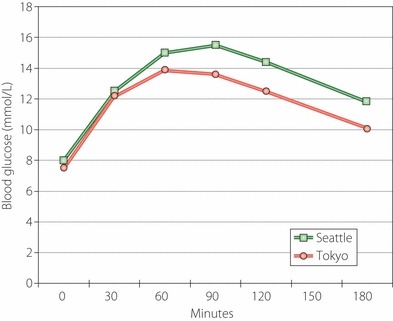
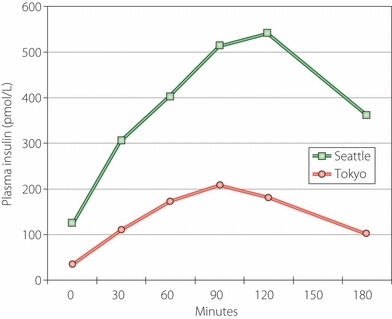
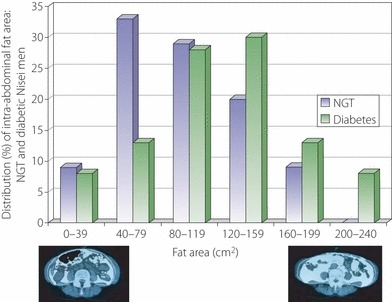
Migrant Japanese populations in both the United States and Brazil have for a long time shown a higher prevalence of type 2 diabetes than in native Japanese, suggesting an interaction of lifestyle and genetic predisposition in the etiology of type 2 diabetes. The overall objective of the Seattle Japanese American Community Diabetes Study was to learn more about the etiology and pathogenesis of type 2 diabetes in Japanese Americans. This metabolically based epidemiologic study included extensive assessments of insulin sensitivity, insulin response, and adiposity with the latter including measurements of body fat distribution by both anthropometry and computed tomography. Because of this, the importance of visceral adiposity as a risk factor for abnormal glucose tolerance, hypertension, coronary heart disease, and the metabolic syndrome was demonstrated. In conjunction with an examination of diet and physical activity patterns, the result was a clearer understanding of the etiology and pathogenesis of type 2 diabetes in Japanese Americans. Wepropose that a lifestyle that fosters increased weight gain, especially in the visceral adipose depot, promotes the development of insulin resistance which in turn exposes an underlying reduced beta-cell reserve in susceptible individuals, resulting in glucose intolerance and eventually in many the development of diabetes. We have shown that it may be possible to delay or prevent the development of diabetes through dietary and exercise interventions in individuals identified as having impaired glucose tolerance. The lessons learned from studying migrant Japanese in Seattle may in many ways be applicable to other populations of Asian origin.
Figures
References
-
- Sloan R. Ethnic distribution of diabetes mellitus in Hawaii. JAMA 1963; 183: 419–424 - PubMed
-
- Kagan A, Harris BR, Winkelstein W Jr, et al. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii, and California: demographic, physical, dietary and biochemical characteristics. J Chronic Dis 1974; 27: 345–364 - PubMed
-
- Kawate R, Yamakido M, Nishimoto Y, et al. Migrant studies?among the Japanese in Hiroshima and Hawaii In: Waldhausl WK (ed). Diabetes 1979. Proc 10th Congr Int Diab Fed. Excerpta Med, Amsterdam, 1980; 526–531
-
- West K. Diabetes in American Indians and other native populations of the new world. Diabetes 1974; 23: 841–855 - PubMed
-
- National Diabetes Data Group . Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979; 28: 1039–1057 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
