

A comparison of cancer burden and research spending reveals discrepancies in the distribution of research funding
- PMID: 22800364
- PMCID: PMC3411479
- DOI: 10.1186/1471-2458-12-526
A comparison of cancer burden and research spending reveals discrepancies in the distribution of research funding
Abstract
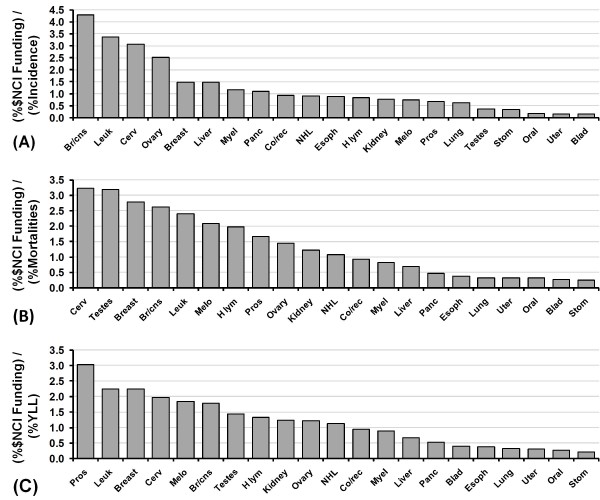
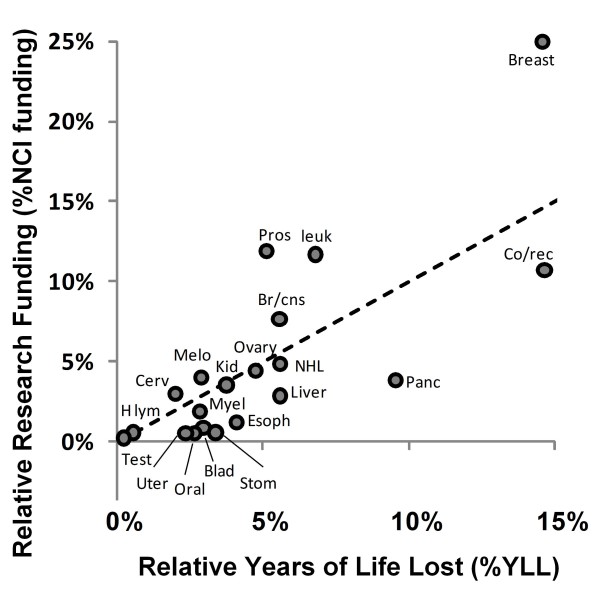
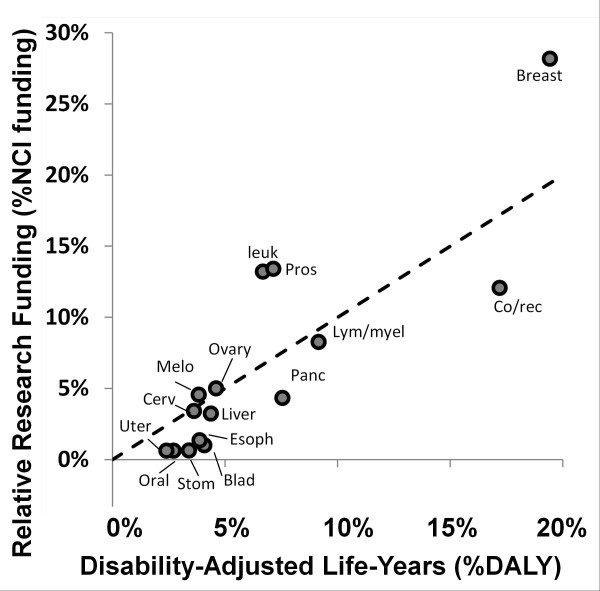
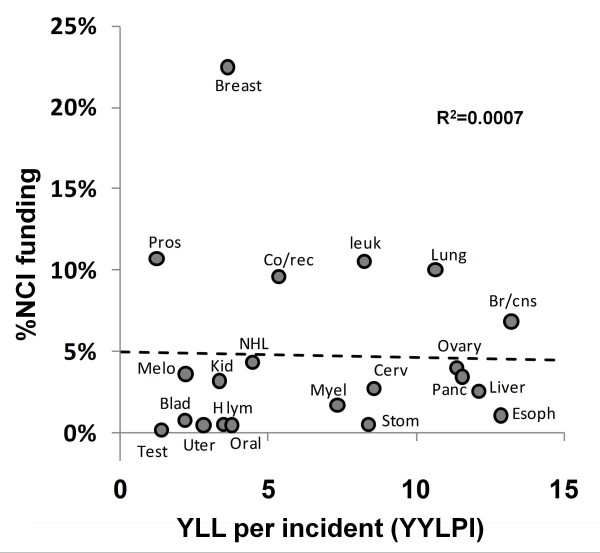
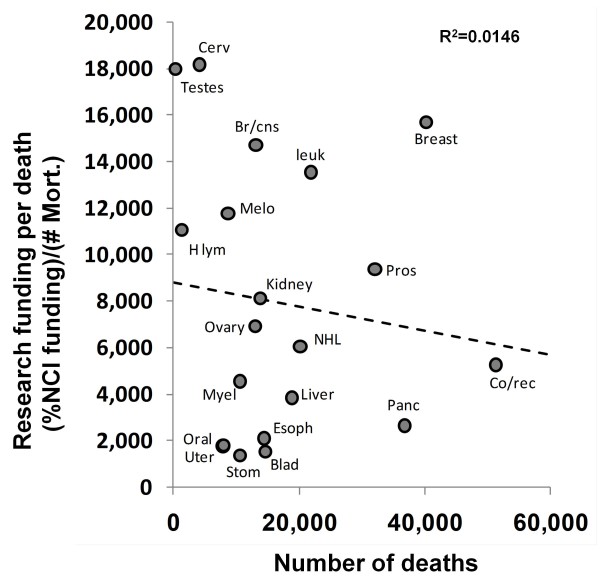
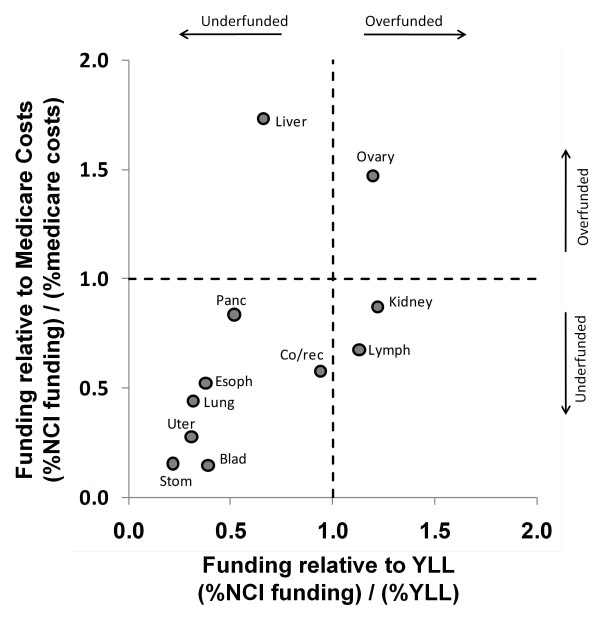
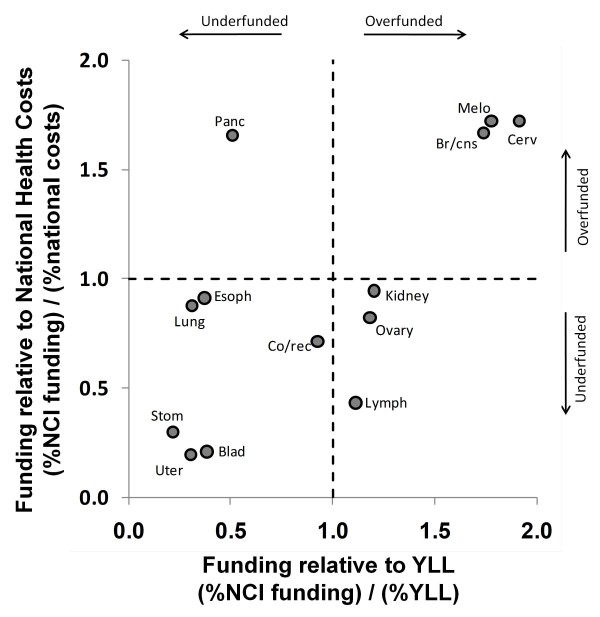
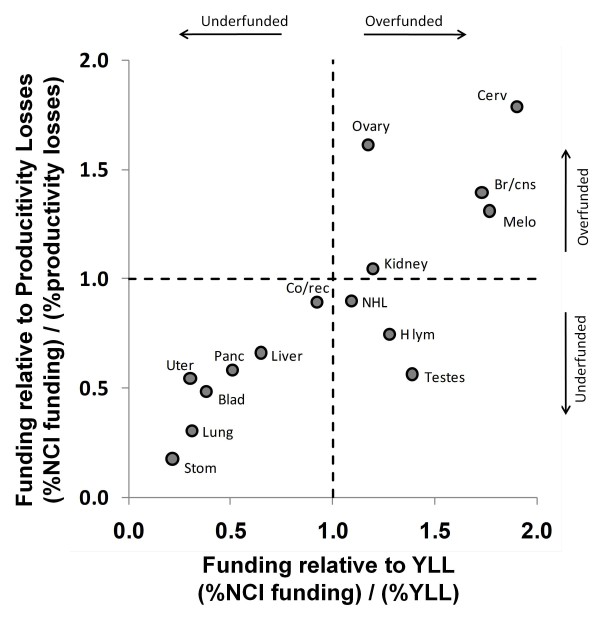
Background: Ideally, the distribution of research funding for different types of cancer should be equitable with respect to the societal burden each type of cancer imposes. These burdens can be estimated in a variety of ways; "Years of Life Lost" (YLL) measures the severity of death in regard to the age it occurs, "Disability-Adjusted Life-Years" (DALY) estimates the effects of non-lethal disabilities incurred by disease and economic metrics focus on the losses to tax revenue, productivity or direct medical expenses. We compared research funding from the National Cancer Institute (NCI) to a variety of burden metrics for the most common types of cancer to identify mismatches between spending and societal burden.
Methods: Research funding levels were obtained from the NCI website and information for societal health and economic burdens were collected from government databases and published reports. We calculated the funding levels per unit burden for a wide range of different cancers and burden metrics and compared these values to identify discrepancies.
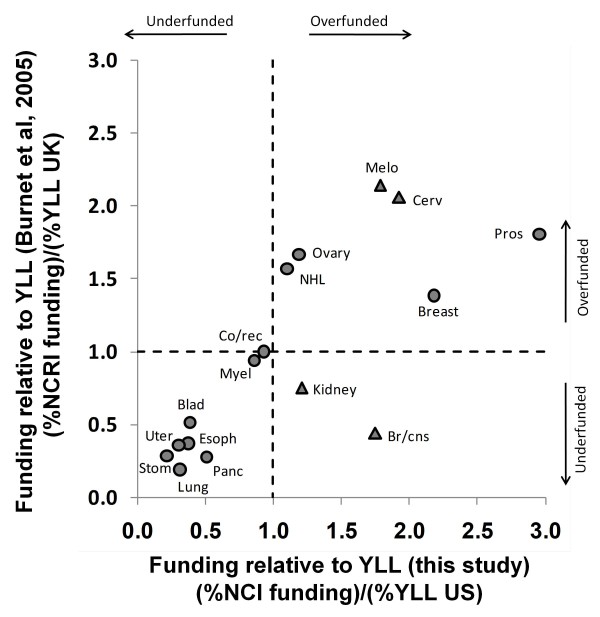
Results: Our analysis reveals a considerable mismatch between funding levels and burden. Some cancers are funded at levels far higher than their relative burden suggests (breast cancer, prostate cancer, and leukemia) while other cancers appear underfunded (bladder, esophageal, liver, oral, pancreatic, stomach, and uterine cancers).
Conclusions: These discrepancies indicate that an improved method of health care research funding allocation should be investigated to better match funding levels to societal burden.
Figures
References
-
- Murphy SL, Xu J, Kochanek KD. Deaths: Preliminary Data for. Natl Vital Stat Rep. 2010;60(4):51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
