

Equivocal p16 immunostaining in squamous cell carcinoma of the head and neck: staining patterns are suggestive of HPV status
- PMID: 22801997
- PMCID: PMC3500888
- DOI: 10.1007/s12105-012-0382-3
Equivocal p16 immunostaining in squamous cell carcinoma of the head and neck: staining patterns are suggestive of HPV status
Abstract
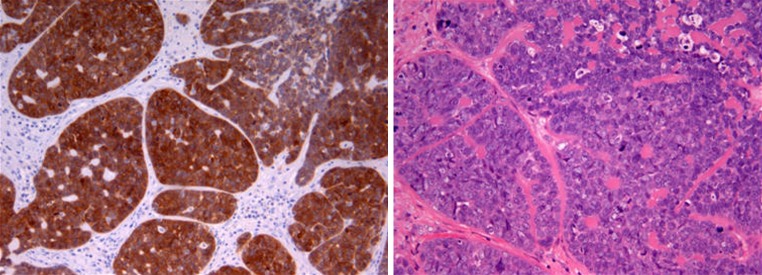
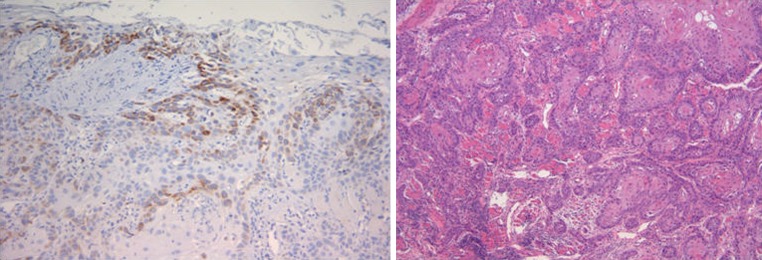
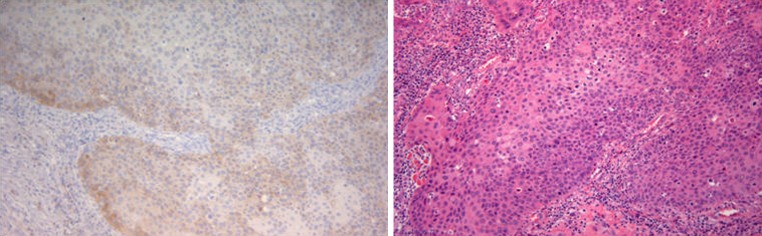
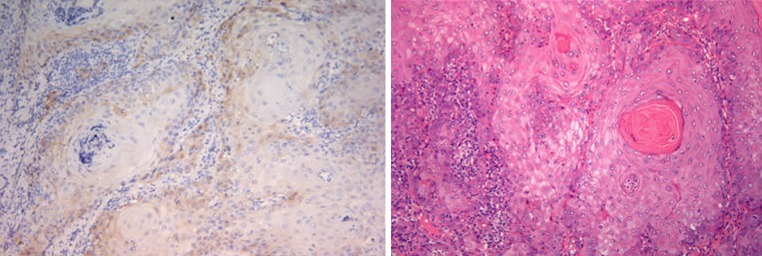
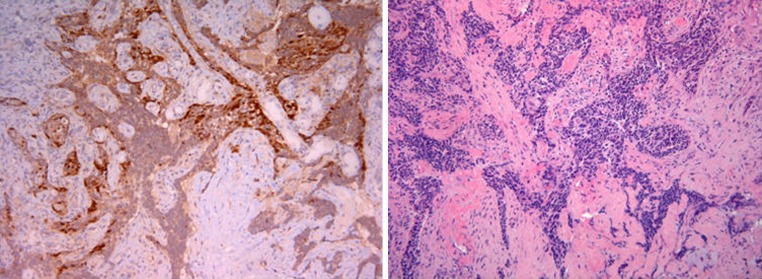
p16 immunohistochemistry (IHC) is commonly used as a surrogate marker for human papillomavirus (HPV) detection in squamous cell carcinomas of the head and neck (SCCHN). However, the HPV status of tumors not staining strongly for p16 is difficult to interpret and may require the use of PCR, not available in all laboratories, as a final arbiter. We aim to determine if staining pattern in equivocal p16 staining and correlation to the percentage of positively stained tumor cells is predictive of HPV status. A retrospective review was performed on all SCCHN that underwent p16 IHC and PCR in our institution from 2007 to 2010. Descriptors of staining pattern in the original IHC report were retrieved. All available IHC slides were reviewed and reclassified using consensus staining pattern descriptors. Original and reclassified descriptors were compared to the final PCR HPV status for statistical significance using the χ(2) test. An estimate of the percentage of tumor cells that showed any form of staining was performed. Thirty-two SCCHN cases that underwent PCR HPV testing had equivocal p16 IHC results. Twenty-six cases available for review were reclassified into four staining patterns. Comparing age, sex, tumor site and diagnosis to HPV PCR status showed no statistically significant findings. However, comparing original descriptors to HPV status was statistically significant with isolated staining associated with negative HPV status (p = 0.0002). Analysis using reclassified descriptors showed strong association of membranous/cytoplasmic staining of isolated cells with negative HPV status and faint, diffuse nuclear and cytoplasmic staining with positive HPV status (p = 0.00006). HPV-negative cases with the former pattern had no more than 30 % positively-stained tumor cells and HPV-positive cases with the latter pattern had 50-90 % positively-stained cells. Our results suggest that pattern of staining in p16 IHC is associated with HPV status. For instance, a diffuse nuclear and cytoplasmic staining pattern, regardless of intensity, is associated with HPV positivity. The HPV-positive cases determined by staining pattern were also associated with a higher percentage of stained tumor cells.
Figures
Similar articles
-
Heterogeneity of p16 immunohistochemistry and increased sensitivity of RNA in situ hybridization in cytology specimens of HPV-related head and neck squamous cell carcinoma.Cancer Cytopathol. 2019 Oct;127(10):632-642. doi: 10.1002/cncy.22178. Epub 2019 Sep 11. Cancer Cytopathol. 2019. PMID: 31509355
-
P16(INK4A) immunostaining is a strong indicator for high-risk-HPV-associated oropharyngeal carcinomas and dysplasias, but is unreliable to predict low-risk-HPV-infection in head and neck papillomas and laryngeal dysplasias.Int J Cancer. 2014 May 1;134(9):2108-17. doi: 10.1002/ijc.28534. Epub 2013 Oct 21. Int J Cancer. 2014. PMID: 24127203
-
Simultaneous p53 and p16 Immunostaining for Molecular Subclassification of Head and Neck Squamous Cell Carcinomas.Head Neck Pathol. 2024 Aug 7;18(1):73. doi: 10.1007/s12105-024-01680-z. Head Neck Pathol. 2024. PMID: 39110300 Free PMC article.
-
p16, HPV, and Cetuximab: What Is the Evidence?Oncologist. 2017 Jul;22(7):811-822. doi: 10.1634/theoncologist.2016-0433. Epub 2017 May 18. Oncologist. 2017. PMID: 28526718 Free PMC article. Review.
-
Is p16 an adequate surrogate for human papillomavirus status determination?Curr Opin Otolaryngol Head Neck Surg. 2017 Apr;25(2):108-112. doi: 10.1097/MOO.0000000000000341. Curr Opin Otolaryngol Head Neck Surg. 2017. PMID: 28141601 Review.
Cited by
-
HPV Detection in Head and Neck Squamous Cell Carcinomas: What Is the Issue?Front Oncol. 2020 Sep 15;10:1751. doi: 10.3389/fonc.2020.01751. eCollection 2020. Front Oncol. 2020. PMID: 33042820 Free PMC article. Review.
-
Comparative Evaluation of Immunohistochemical Expression of p16 with p16 Microsatellite Marker by PCR in Surgical Margins of Oral Squamous Cell Carcinoma.Indian J Otolaryngol Head Neck Surg. 2019 Oct;71(Suppl 1):716-723. doi: 10.1007/s12070-018-1517-y. Epub 2018 Oct 31. Indian J Otolaryngol Head Neck Surg. 2019. PMID: 31742049 Free PMC article.
-
Assessment of immunohistochemical expression of p16 in head and neck squamous cell carcinoma and their correlation with clinicopathological parameters.J Oral Maxillofac Pathol. 2021 Jan-Apr;25(1):74-81. doi: 10.4103/jomfp.JOMFP_252_20. Epub 2021 May 14. J Oral Maxillofac Pathol. 2021. PMID: 34349415 Free PMC article.
-
The prevalence of human papillomavirus in oropharyngeal cancer in a New Zealand population.PLoS One. 2017 Oct 19;12(10):e0186424. doi: 10.1371/journal.pone.0186424. eCollection 2017. PLoS One. 2017. PMID: 29049330 Free PMC article.
-
Current and future techniques for human papilloma virus (HPV) testing in oropharyngeal squamous cell carcinoma.Eur Arch Otorhinolaryngol. 2017 Jul;274(7):2675-2683. doi: 10.1007/s00405-017-4503-1. Epub 2017 Mar 11. Eur Arch Otorhinolaryngol. 2017. PMID: 28285422 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
