

Duodenal adenocarcinoma arising from a pyloric gland adenoma with a brief review of the literature
- PMID: 22802482
- PMCID: PMC3028104
- DOI: 10.1136/bcr.10.2010.3385
Duodenal adenocarcinoma arising from a pyloric gland adenoma with a brief review of the literature
Abstract
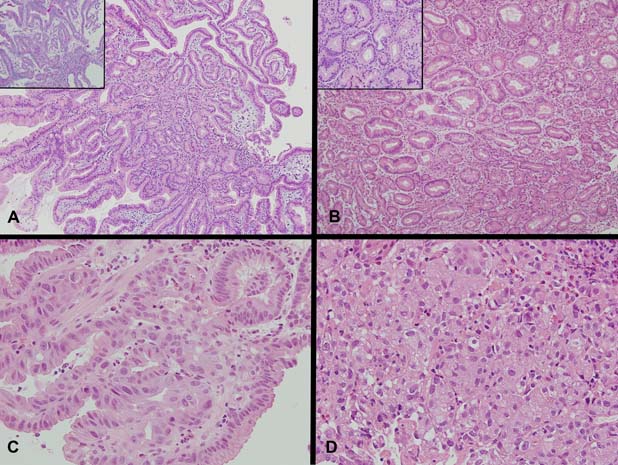
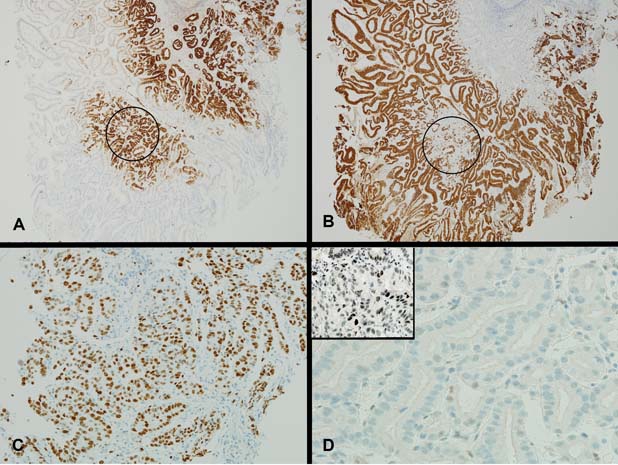
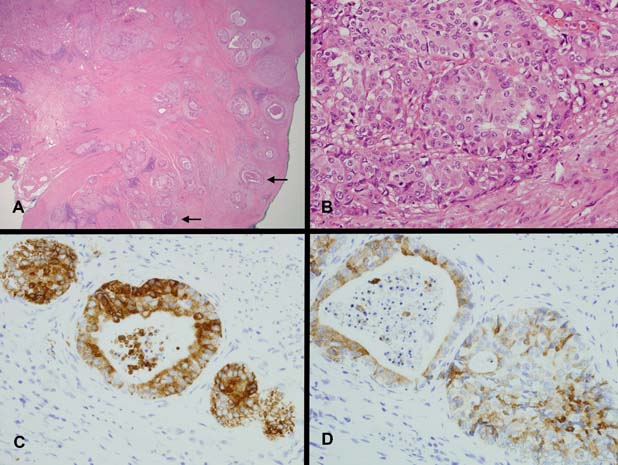
Pyloric gland-type adenoma of the duodenum with documented malignant progression is rare. A case is presented of an 87-year-old man with bloating and nausea, who on investigation was found to have a polyp on the anteroinferior wall of the duodenal cap. Histologic examination of the polyp showed features of a pyloric gland adenoma (PGA) demonstrating the full spectrum of progression from low- to high-grade dysplasia and finally invasive adenocarcinoma. The carcinoma showed gastric-type differentiation highlighted by its mucin immunohistochemistry profile and was of advanced stage with lymph node metastasis. The literature on PGAs and the little documentations on progression to carcinoma in duodenal PGAs are reviewed.
Conflict of interest statement
Figures
References
-
- Chen ZM, Scudiere JR, Abraham SC, et al. Pyloric gland adenoma: an entity distinct from gastric foveolar type adenoma. Am J Surg Pathol 2009;33:186–93 - PubMed
-
- Vieth M, Kushima R, Borchard F, et al. Pyloric gland adenoma: a clinico-pathological analysis of 90 cases. Virchows Arch 2003;442:317–21 - PubMed
-
- Kushima R, Rüthlein HJ, Stolte M, et al. ‘Pyloric gland-type adenoma’ arising in heterotopic gastric mucosa of the duodenum, with dysplastic progression of the gastric type. Virchows Arch 1999;435:452–7 - PubMed
-
- Kushima R, Vieth M, Mukaisho K, et al. Pyloric gland adenoma arising in Barrett's esophagus with mucin immunohistochemical and molecular cytogenetic evaluation. Virchows Arch 2005;446:537–41 - PubMed
-
- Vieth M, Kushima R, de Jonge JP, et al. Adenoma with gastric differentiation (so-called pyloric gland adenoma) in a heterotopic gastric corpus mucosa in the rectum. Virchows Arch 2005;446:542–5 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous