

Thrombotic microangiopathy and associated renal disorders
- PMID: 22802583
- PMCID: PMC3398067
- DOI: 10.1093/ndt/gfs279
Thrombotic microangiopathy and associated renal disorders
Abstract
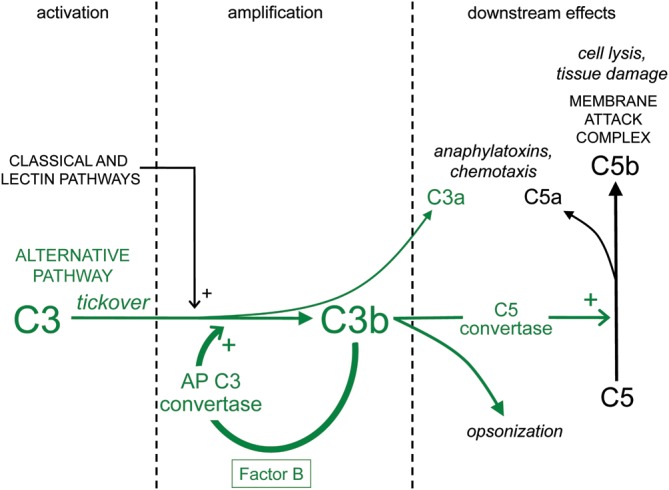
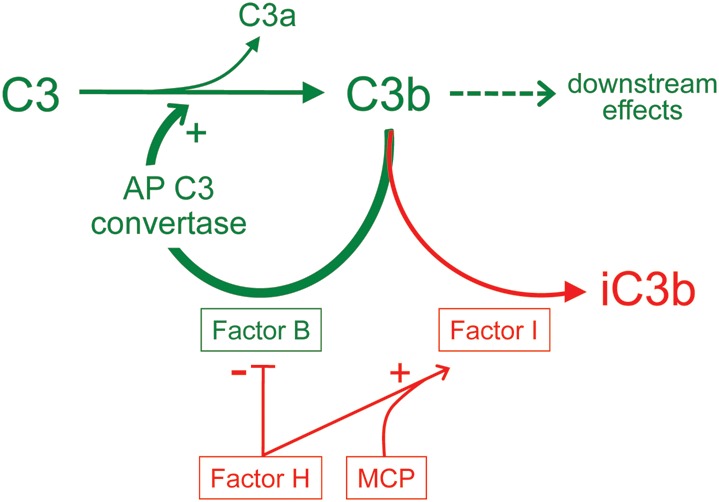
Thrombotic microangiopathy (TMA) is a pathological process involving thrombocytopenia, microangiopathic haemolytic anaemia and microvascular occlusion. TMA is common to haemolytic uraemic syndrome (HUS) associated with shiga toxin or invasive pneumococcal infection, atypical HUS (aHUS), thrombotic thrombocytopenic purpura (TTP) and other disorders including malignant hypertension. HUS complicating infection with shiga toxin-producing Escherichia coli (STEC) is a significant cause of acute renal failure in children worldwide, occurring sporadically or in epidemics. Studies in aHUS have revealed genetic and acquired factors leading to dysregulation of the alternative complement pathway. TTP has been linked to reduced activity of the ADAMTS13 cleaving protease (typically with an autoantibody to ADAMTS13) with consequent disruption of von Willebrand factor multimer processing. However, the convergence of pathogenic pathways and clinical overlap create diagnostic uncertainty, especially at initial presentation. Furthermore, recent developments are challenging established management protocols. This review addresses the current understanding of molecular mechanisms underlying TMA, relating these to clinical presentation with an emphasis on renal manifestations. A diagnostic and therapeutic approach is presented, based on international guidelines, disease registries and published trials. Early treatment remains largely empirical, consisting of plasma replacement/exchange with the exception of childhood STEC-HUS or pneumococcal sepsis. Emerging therapies such as the complement C5 inhibitor eculizumab for aHUS and rituximab for TTP are discussed, as is renal transplantation for those patients who become dialysis-dependent as a result of aHUS.
Figures
References
-
- Ariceta G, Besbas N, Johnson S, et al. Guideline for the investigation and initial therapy of diarrhea-negative hemolytic uremic syndrome. Pediatr Nephrol. 2009;24:687–696. - PubMed
-
- Brain MC, Dacie JV, Hourihane DO. Microangiopathic haemolytic anaemia: the possible role of vascular lesions in pathogenesis. Br J Haematol. 1962;8:358–374. - PubMed
-
- Park YA, Waldrum MR, Marques MB. Platelet count and prothrombin time help distinguish thrombotic thrombocytopenic purpura-hemolytic uremic syndrome from disseminated intravascular coagulation in adults. Am J Clin Pathol. 2010;133:460–465. - PubMed
-
- Moschcowitz E. An acute febrile pleiochromic anemia with hyaline thrombosis of the terminal arterioles and capillaries: an undescribed disease. Arch Intern Med. 1925;36:89–93. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
