

Quality improvement initiative to reduce serious safety events and improve patient safety culture
- PMID: 22802607
- PMCID: PMC3408689
- DOI: 10.1542/peds.2011-3566
Quality improvement initiative to reduce serious safety events and improve patient safety culture
Abstract
Background and objective: Many thousands of patients die every year in the United States as a result of serious and largely preventable safety events or medical errors. Safety events are common in hospitalized children. We conducted a quality improvement initiative to implement cultural and system changes with the goal of reducing serious safety events (SSEs) by 80% within 4 years at our large, urban pediatric hospital.
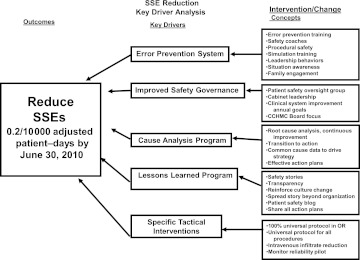
Methods: A multidisciplinary SSE reduction team reviewed the safety literature, examined recent SSEs, interviewed internal leaders, and visited other leading organizations. Senior hospital leaders provided oversight, monitored progress, and helped to overcome barriers. Interventions focused on: (1) error prevention; (2) restructuring patient safety governance; (3) a new root cause analysis process and a common cause database; (4) a highly visible lessons learned program; and (5) specific tactical interventions for high-risk areas. Our outcome measures were the rate of SSEs and the change in patient safety culture.
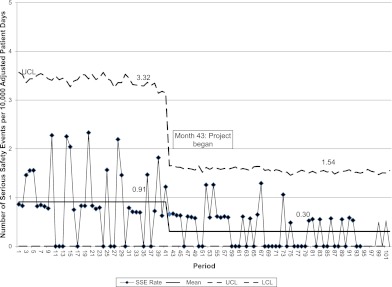
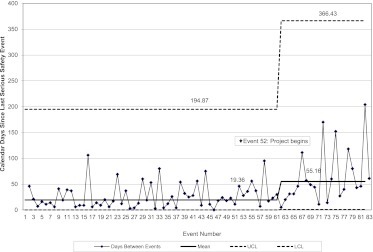
Results: SSEs per 10000 adjusted patient-days decreased from a mean of 0.9 at baseline to 0.3 (P < .0001). The days between SSEs increased from a mean of 19.4 at baseline to 55.2 (P < .0001). After a worsening of patient safety culture outcomes in the first year of intervention, significant improvements were observed between 2007 and 2009.
Conclusions: Our multifaceted approach was associated with a significant and sustained reduction of SSEs and improvements in patient safety culture. Multisite studies are needed to better understand contextual factors and the significance of specific interventions.
Figures
References
-
- Institute of Medicine, Committee on Quality Health Care in America Crossing the Quality Chasm—A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001
-
- Institute of Medicine, Committee on Quality of Health Care in America To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000
-
- Leape LL. Scope of problem and history of patient safety. Obstet Gynecol Clin North Am. 2008;35(1):1–10, vii - PubMed
-
- Luria JW, Muething SE, Schoettker PJ, Kotagal UR. Reliability science and patient safety. Pediatr Clin North Am. 2006;53(6):1121–1133 - PubMed
-
- Weick KE, Sutcliffe KM, Obstfeld D. Organizing for high reliability: processes of collective mindfulness. Res Organ Behav. 1999;21:81–123
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
