

Intraosseous lipomas: A report of six cases and a review of literature
- PMID: 22802856
- PMCID: PMC3389946
Intraosseous lipomas: A report of six cases and a review of literature
Abstract
Background: Intraosseous lipoma is a very rare lesion, which constitutes not more than 0.1% of bone tumors. The introduction of cross-sectional imaging, especially MRI, seems to have increased the detection rate of these lesions.
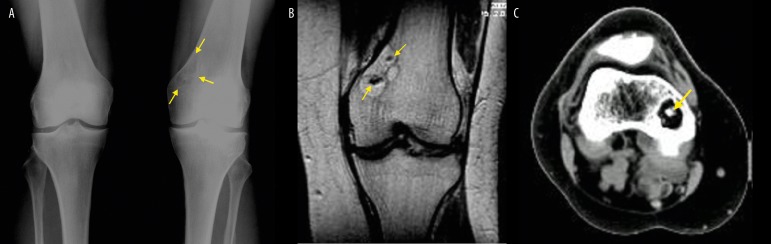
Case report: The authors presented 6 cases of intraosseous lipomas in bones of the lower extremities. All lesions were detected incidentally and presented radiographically as radiolucent lesions with sclerotic borders and internal trabeculations. One lesion caused bone expansion. CT and MRI identified fatty tissue in all lesions. Cystic degeneration was present in one lesion and dystrophic calcifications in two.
Discussion: The radiographic appearance of intraosseous lipomas is not characteristic and requires differential diagnostics conducted for a long time. However, CT and MRI allow for a tissue-specific diagnosis. The detection of a predominant fatty component in a lesion confirms its benign character and no further diagnostic work-up is required.
Keywords: bone tumor; imaging; intraosseous lipoma.
Figures







References
-
- Schajowicz F. Tumors and tumorlike lesions of bone: pathology, radiology and treatment. 2nd ed. Springer-Verlag; 1994.
-
- Dahlin DC, Unni KK. Bone tumors: general aspects and data on 8,542 cases. 4th ed. Charles C Thomas; Springfield IL: p. 1986.
-
- Campbell RSD, Grainger AJ, Mangham DC, et al. Intraosseus lipoma: report of 35 new cases and a review of the literature. Skeletal Radiol. 2003;32:209–22. - PubMed
-
- Milgram JW. Intraosseous lipomas. A clinicopathologic study of 66 cases. Clin Orthop. 1988;231:277–302. - PubMed
-
- Greenspan A, Jundt G, Remagen W. Diagnostyka różnicowa w onkologii ortopedycznej. Medipage. 2008:438–42. [in Polish]
Publication types
LinkOut - more resources
Full Text Sources