

Relationships among initial hospital triage, disease progression and mortality in community-acquired pneumonia
- PMID: 22805170
- PMCID: PMC3544548
- DOI: 10.1111/j.1440-1843.2012.02225.x
Relationships among initial hospital triage, disease progression and mortality in community-acquired pneumonia
Abstract
Background and objective: Appropriate triage of patients with community-acquired pneumonia (CAP) may improve morbidity, mortality and use of hospital resources. Worse outcomes from delayed intensive care unit (ICU) admission have long been suspected but have not been verified.
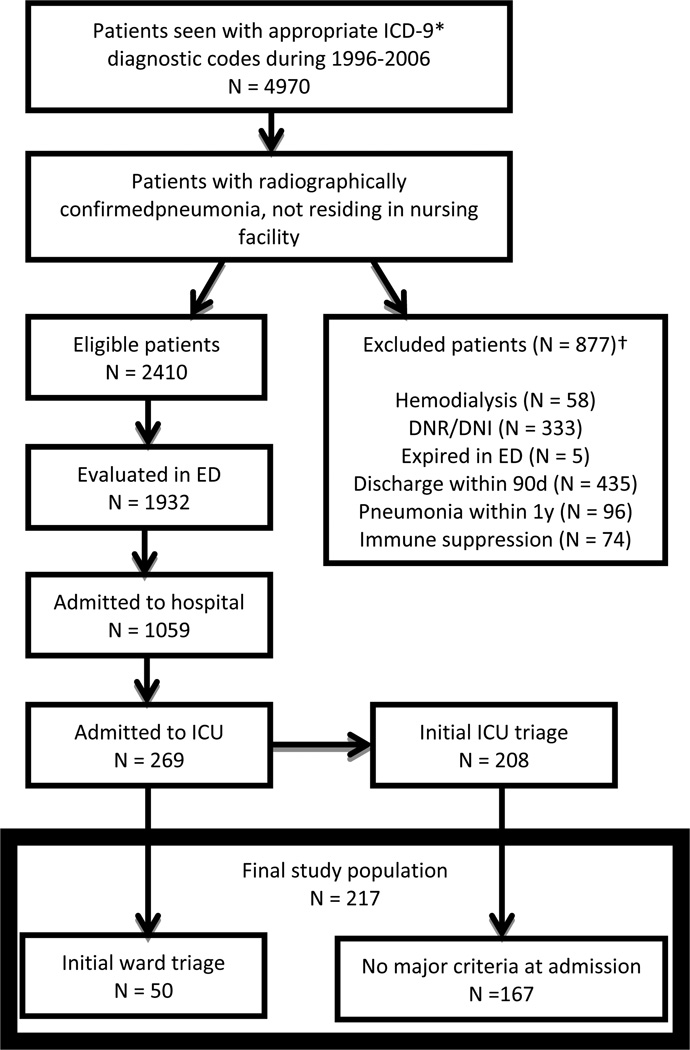
Methods: In a retrospective study of consecutive patients with CAP admitted from 1996-2006 to the ICUs of a tertiary care hospital, we measured serial severity scores, intensive therapies received, ICU-free days, and 30-day mortality. Primary outcome was mortality. We developed a regression model of mortality with ward triage (and subsequent ICU transfer within 72 h) as the predictor, controlled by propensity for ward triage and radiographic progression.
Results: Of 1059 hospital-admitted patients, 269 (25%) were admitted to the ICU during hospitalization. Of those, 167 were directly admitted to the ICU without current requirement for life support, while 61 (23%) were initially admitted to the hospital ward, 50 of those undergoing ICU transfer within 72 h. Ward triage was associated with increased mortality (OR 2.6, P = 0.056) after propensity adjustment. The effect was less (OR 2.2, P = 0.12) after controlling for radiographic progression. The effect probably increased (OR 4.1, P = 0.07) among patients with ≥ 3 severity predictors at admission.
Conclusions: Initial ward triage among patients transferred to the ICU is associated with twofold higher 30-day mortality. This effect is most apparent among patients with ≥ 3 severity predictors at admission and is attenuated by controlling for radiographic progression. Intensive monitoring of ward-admitted patients with CAP seems warranted. Further research is needed to optimize triage in CAP.
© 2012 The Authors. Respirology © 2012 Asian Pacific Society of Respirology.
Figures
Similar articles
-
Lactate to albumin ratio as a determinant of intensive care unit admission and mortality in hospitalized patients with community-acquired pneumonia.BMC Pulm Med. 2025 May 9;25(1):224. doi: 10.1186/s12890-025-03698-7. BMC Pulm Med. 2025. PMID: 40346545 Free PMC article.
-
Efficacy and significance of various scores for pneumonia severity in the management of patients with community-acquired pneumonia in China.Chin Med J (Engl). 2012 Feb;125(4):639-45. Chin Med J (Engl). 2012. PMID: 22490488
-
Pneumonia severity index class v patients with community-acquired pneumonia: characteristics, outcomes, and value of severity scores.Chest. 2007 Aug;132(2):515-22. doi: 10.1378/chest.07-0306. Epub 2007 May 15. Chest. 2007. PMID: 17505026
-
Guideline adherence for empirical treatment of pneumonia and patient outcome. Treating pneumonia in the Netherlands.Neth J Med. 2013 Dec;71(10):502-7. Neth J Med. 2013. PMID: 24394734 Review.
-
Year in review 2012: Critical Care--management.Crit Care. 2013 Nov 22;17(6):250. doi: 10.1186/cc12759. Crit Care. 2013. PMID: 24438819 Free PMC article. Review.
Cited by
-
Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America.Am J Respir Crit Care Med. 2019 Oct 1;200(7):e45-e67. doi: 10.1164/rccm.201908-1581ST. Am J Respir Crit Care Med. 2019. PMID: 31573350 Free PMC article.
-
Progression of the Radiologic Severity Index predicts mortality in patients with parainfluenza virus-associated lower respiratory infections.PLoS One. 2018 May 17;13(5):e0197418. doi: 10.1371/journal.pone.0197418. eCollection 2018. PLoS One. 2018. PMID: 29771962 Free PMC article.
-
ICU Utilization After Implementation of Minor Severe Pneumonia Criteria in Real-Time Electronic Clinical Decision Support.Crit Care Med. 2024 Mar 1;52(3):e132-e141. doi: 10.1097/CCM.0000000000006163. Epub 2023 Dec 29. Crit Care Med. 2024. PMID: 38157205 Free PMC article.
-
Severe community-acquired pneumonia: timely management measures in the first 24 hours.Crit Care. 2016 Aug 28;20(1):237. doi: 10.1186/s13054-016-1414-2. Crit Care. 2016. PMID: 27567896 Free PMC article. Review.
-
A Broad Learning System to Predict the 28-Day Mortality of Patients Hospitalized with Community-Acquired Pneumonia: A Case-Control Study.Comput Math Methods Med. 2022 Mar 4;2022:7003272. doi: 10.1155/2022/7003272. eCollection 2022. Comput Math Methods Med. 2022. PMID: 35281948 Free PMC article.
References
-
- Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, et al. Deaths: final data for 2006. Natl Vital Stat Rep. 2009;57:1–134. - PubMed
-
- Armstrong GL, Conn LA, Pinner RW. Trends in infectious disease mortality in the United States during the 20th century. Jama. 1999;281:61–66. - PubMed
-
- Singanayagam A, Chalmers JD, Hill AT. Severity assessment in community-acquired pneumonia: a review. QJM. 2009 - PubMed
-
- Marston BJ, Plouffe JF, File TM, Jr, Hackman BA, Salstrom SJ, et al. Incidence of community-acquired pneumonia requiring hospitalization. Results of a population-based active surveillance Study in Ohio. The Community-Based Pneumonia Incidence Study Group. Arch Intern Med. 1997;157:1709–1718. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
