

To be screened or not to be screened? Modeling the consequences of PSA screening for the individual
- PMID: 22805324
- PMCID: PMC3425982
- DOI: 10.1038/bjc.2012.317
To be screened or not to be screened? Modeling the consequences of PSA screening for the individual
Abstract
Background: Screening with prostate-specific antigen (PSA) can reduce prostate cancer mortality, but may advance diagnosis and treatment in time and lead to overdetection and overtreatment. We estimated benefits and adverse effects of PSA screening for individuals who are deciding whether or not to be screened.
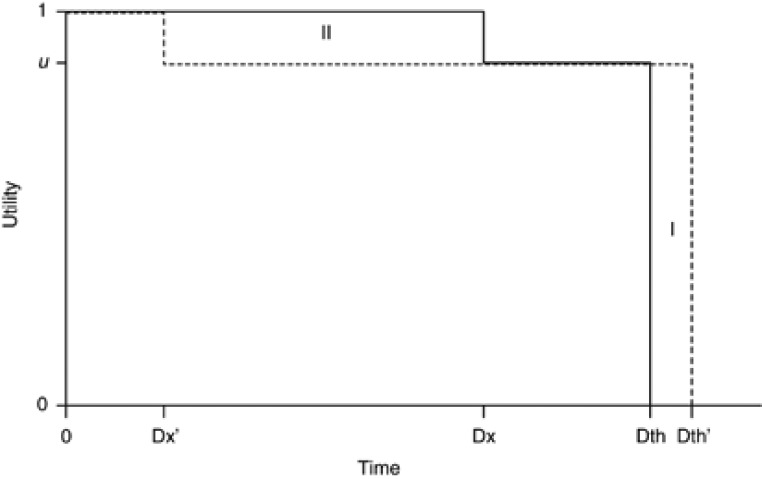
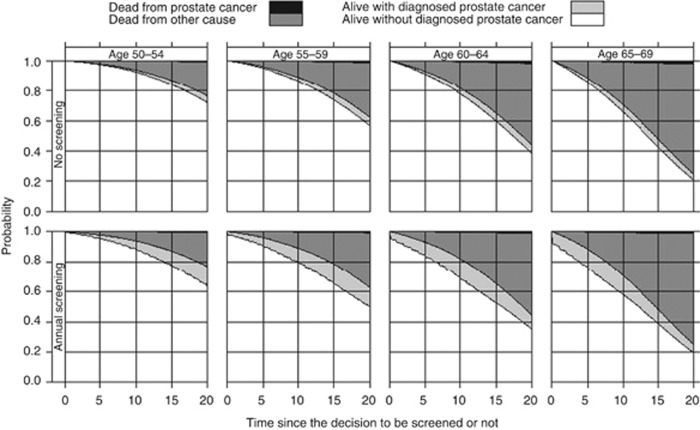
Methods: Using a microsimulation model, we estimated lifetime probabilities of prostate cancer diagnosis and death, overall life expectancy and expected time to diagnosis, both with and without screening. We calculated anticipated loss in quality of life due to prostate cancer diagnosis and treatment that would be acceptable to decide in favour of screening.
Results: Men who were screened had a gain in life expectancy of 0.08 years but their expected time to diagnosis decreased by 1.53 life-years. Of the screened men, 0.99% gained on average 8.08 life-years and for 17.43% expected time to diagnosis decreased by 8.78 life-years. These figures imply that the anticipated loss in quality of life owing to diagnosis and treatment should not exceed 4.8%, for screening to have a positive effect on quality-adjusted life expectancy.
Conclusion: The decision to be screened should depend on personal preferences. The negative impact of screening might be reduced by screening men who are more willing to accept the side effects from treatment.
Figures
References
-
- Albertsen PC, Hanley JA, Fine J (2005) 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA 293: 2095–2101 - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, Garmo H, Stark JR, Busch C, Nordling S, Haggman M, Andersson SO, Bratell S, Spangberg A, Palmgren J, Steineck G, Adami HO, Johansson JE (2011) Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 364: 1708–1717 - PubMed
-
- Carlsson S, Aus G, Bergdahl S, Khatami A, Lodding P, Stranne J, Hugosson J (2011) The excess burden of side-effects from treatment in men allocated to screening for prostate cancer. The Goteborg randomised population-based prostate cancer screening trial. Eur J Cancer 47: 545–553 - PubMed
-
- CBS (2010) Centrale Bureau van Statistieken, http://statline.cbs.nl/StatWeb/publication/?VW=T&DM=SLNL&PA=0379... (accessed 1 February 2012)
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
